


NEJM proves that covid vaccine study methodologies are rigged
sometimes a study winds up proving something far more interesting than it intended.

cliff notes:
when you account for all post booster risk instead of accepting the “booster +12 days” definition the reported efficacy of this study not only vanishes, it inverts.
90%+ VE becomes negative 50-90% for most outcomes.
you cannot trust any study or outcomes assessment that uses these definitions.
and we can demonstrate it here using just their own study data.
the study designs used for covid vaccines are unlike anything i have ever seen (and i read a lot of studies). they use contrived definitions to exclude and transfer huge amounts of risk. long-term readers of this substack will be familiar with this issue and my longstanding description of it as “baysian datacrime.”
in essence, the issue is simple: mRNA covid vaccines and boosters appear to generate a ~2 week window of immuno-suppression post administration. this is clinically validated. this is a period of greatly enhanced risk for the recently vaxxed but the definition used for “vaccinated” or “boosted” is generally “second dose +14 days” and “booster +14 days.” in this manner, they not only avoid having to count the high risk period one must go through to reach “vaccinated” as a part of being vaccinated but often actually add this risk into the previous cohort so the “vaxxed” ascribe immunosuppression enhanced risk to the unvaxxed and the boosted to the double jabbed.
certain waggish internet felines generated this analogy to help make the issue clear.
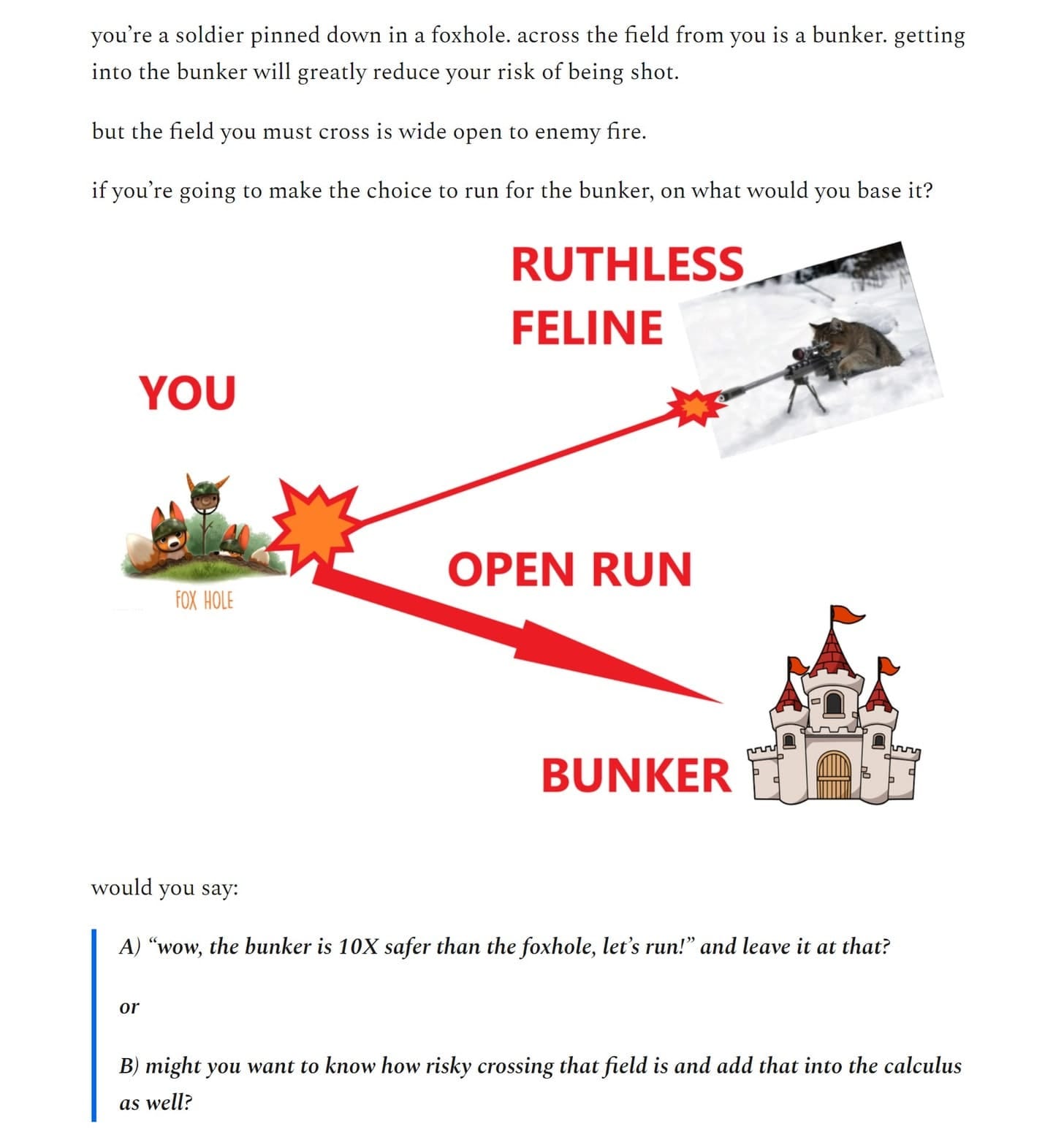
what these studies are doing is accounting ONLY for the safety of the bunker. bad outcomes during the run to get there are counted as “stayed in foxhole.” the numbers they produce are overstated bayesian rigging that take bad outcomes from acting and attribute them to inaction.
it’s why none of the societal outcomes look anything like the studies upon the basis of which these drugs were approved or all this post facto “data analysis.”
the fix is in.
this practice can literally make an immunosuppressant with no clinical efficacy appear to have strong VE. (see second link) it’s one of the most egregious abuses of trial design i’ve ever seen and it appears to be standard practice around the world.
it generated all meaningful reported efficacy in this study in the NEJM (whose referees should have known better or worse, did know better and chose to mislead).
THIS STUDY has been widely used to claim that boosters are extremely effective against covid infection and covid outcomes. it’s a terrible methodology with bad design that is basically unrecoverable right from the start and relies on 20 kinds of “adjustment” that are not made transparent in their assumptions and math.
what they SHOULD have done was cohort match 2 groups by risk at one point in time and compare them across the same temporal interval counting all outcomes from the moment you got a booster in the boosted group. tellingly, no one seems to do this.
one of a cynical bent might be tempted to ask some pointy questions about why…
so, like a feline penn and teller, let me show you why and how the trick is done.

the phrase “We used Poisson regression models to estimate rate ratios after adjusting for possible confounding factors” means: these cohorts were in no way matched. this was not a prospective trial nor randomized. they went back through past data of people who for unknown reasons selected to get boosters or not and who did so at varying times over which disease prevalence varied greatly as did the % of the population with acquired immunity and the overall testing level. there was no control for pre-existing risk from comorbidity etc or even for timing of the inoculation.
it was all mucked with post facto. you can drive a truck through assumptive poisson error and manipulation.
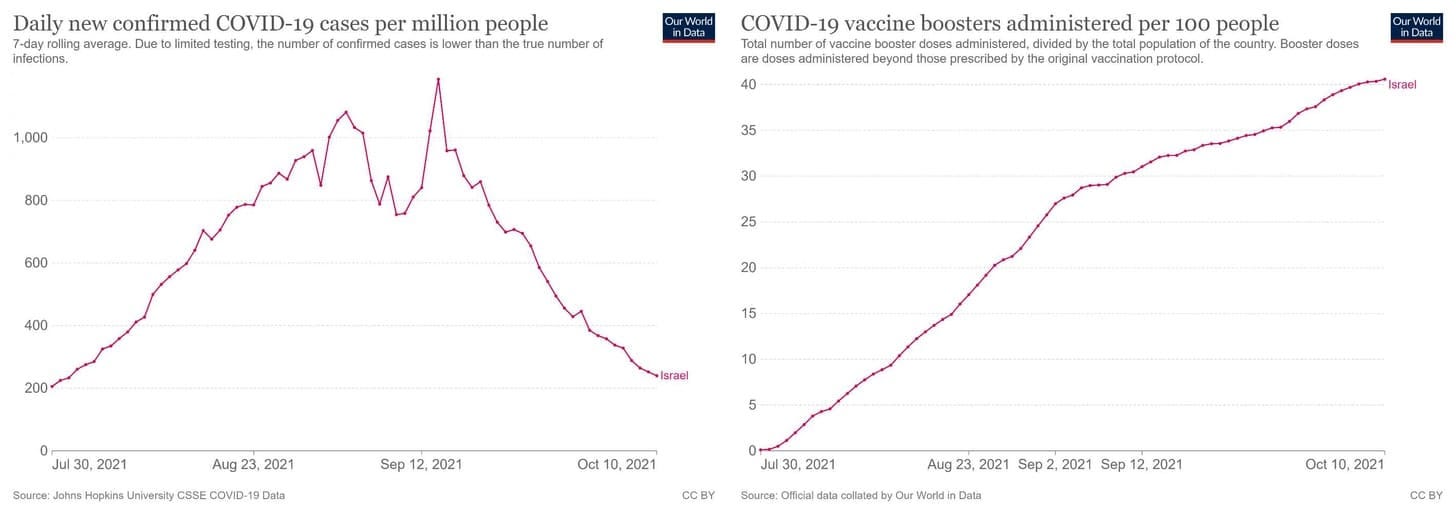
this study began with 0% boosted and ran to 40%. so the meat of the boosted person days were in a period where pre-existing immunity was materially higher. (14% of pop with “confirmed cases” at end of period vs 9% at beginning, a 56% increase, though obviously this is a rough approximation and a large undercount as most cases are not confirmed)
this alone adds unrecoverable bias to the study (and was not, best i can tell, accounted for in the poisson at all)
so far so “not very interesting.”
but what it CAN show is interesting.
it can show just how rigged the trial designs are because of their definitions of “boosted.” and that makes it fun.
studies that discredit themselves by accident are my favorite kind.
so let’s dig a bit deeper.
there are 2 key tables from which we may extract information as they have delineated “person days at risk (PDAR) by cohort” and thus generate meaningful comparison. (maddeningly, the more age delineated and complete table 1 uses %’s of PDAR but never provides a base number.)
this table purports to show a huge drop in cases from “double jabbed” to “boosted.” the rate ratio runs from 9 to 17.2. this corresponds to and 89-96% vaccine efficacy range.
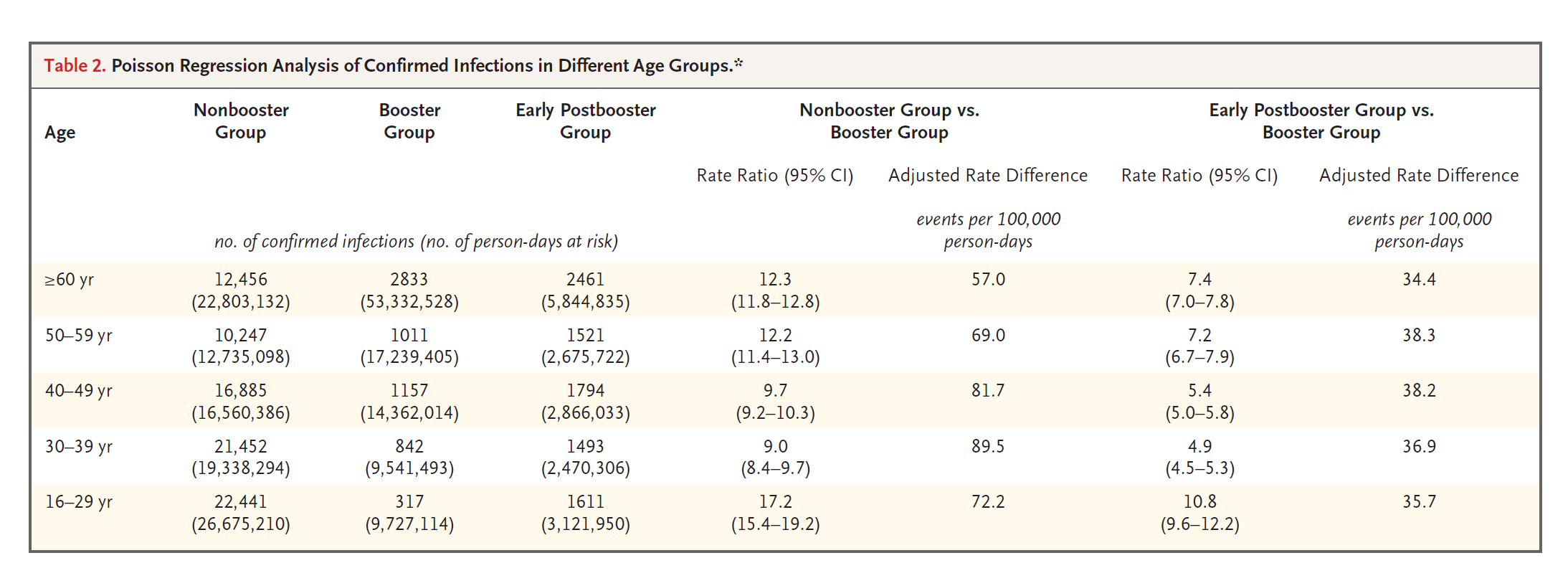
that sounds incredibly effective. but it’s not.
it’s rigged and this table proves it.
to see this, we must examine all the groups. the “early postbooster group” changes everything.
the definitions are:
double vaccinated: got second dose 5 or more months ago
boosted: got a booster more than 12 days ago.
early postbooster: got a booster 3-7 days ago.
and from this, we can start to do some more complete risk assessment. i have no access to the raw data or the poisson fishiness they used to adjust it, so i’m just going to work from the rawest tabular data they provide.
early post booster is “running across the field of fire” as above.
you have to go through days 3-7 to get to post day 12. this is tautological. of course, you also have to go through days 1-2 and 8-12. so this oddly shaped 5 day window is not a complete accounting of the post booster risk. it’s only 42% of the 12 days at risk. why they chose this odd timeframe is anyone’s guess, but “providing a full accounting of real outcomes data” is not it.
so let’s see if we can adjust for this, shall we?
clearly, we can add the risk from early postbooster to boosted. that’s unarguable. we can also prorate it and say, well, if that’s 5 days then 12 days would be ~2.4X more. this gets assumptive, but is probably not far off. it might be too high, or if these outcomes are front or back-end loaded, this adjustment could well be too low. pro-rating is about the best we can do with what we have.
and the results get VERY interesting and turn this study’s claims on their head.
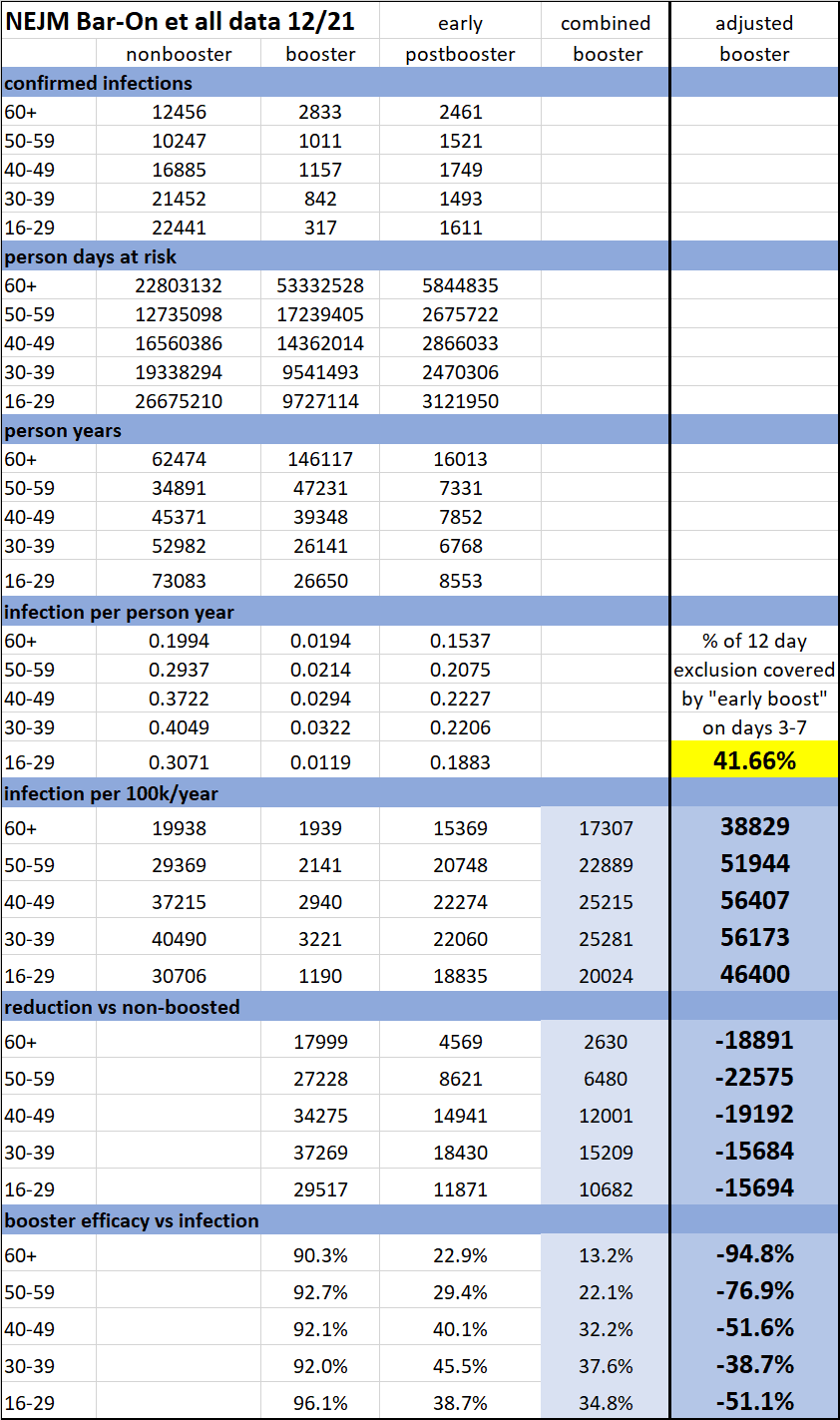
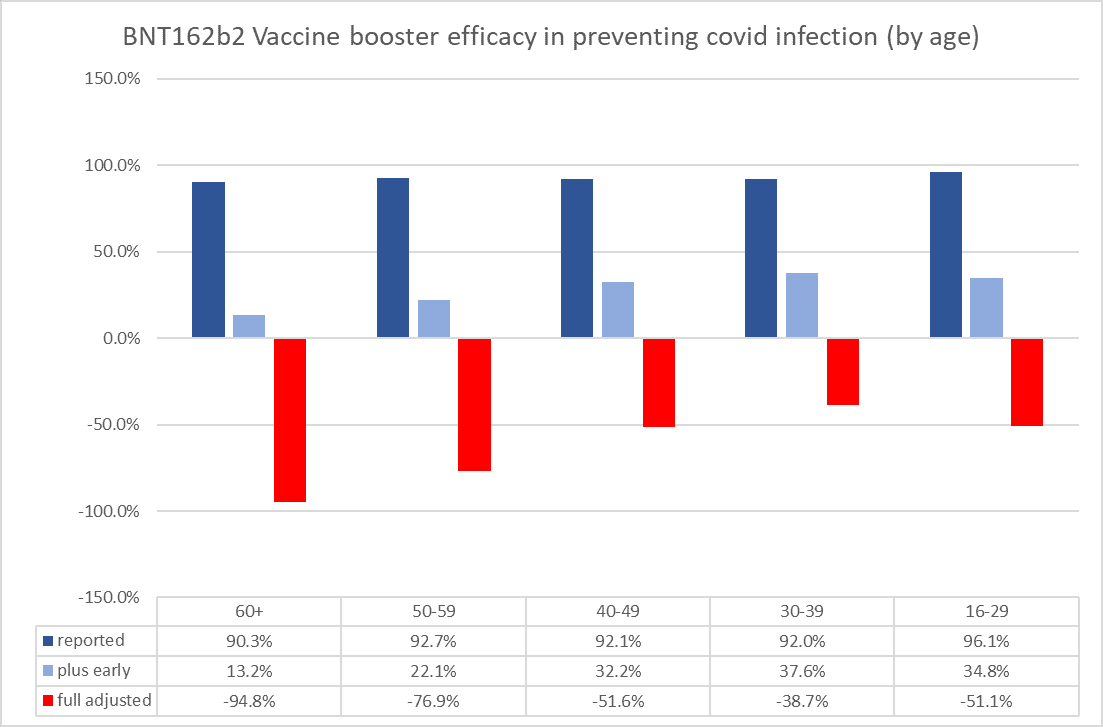
i converted all data to infections per 100k people per year to make it comparable and summative.
i then added early prebooster to booster. as can be seen, the drop in purported vaccine efficacy is precipitous. in over 60’s, 90% drops to 13%. and this much is unarguable.
( the daily risk level of the early postbooster is on the order of 10X more that of the boosted after day 12. small wonder one seeking to show efficacy would want it excluded…)
i then adjusted this data to reflect the full 12 day risk window instead of the 5 day keyhole the study authors used by pro-rating that effect (and assuming it is constant across the 12 days).
doing this drives all VE sharply negative.
and this shows you what a rig job these studies are based on this one definitional trick alone. (and we have not even tried to account for the possible adding of this risk to the other cohorts or any other sneakery.)
for the sake of completeness, the keyhole of 5 of 12 days is 42% of days at risk. for any number under 59% all values flip negative so those 5 days would need to be twice or more the risk of the other 7 days on a per person per day at risk basis for VE to even get back to zero. this is a wide margin of plausibility for “all effect if from risk shifting.”
despite that seeming margin, some will doubtless take exception to this vast alteration in outcomes and so i would like to validate it using independent check.
first, one important concept:
the figures above are rigged in another way: this is a comparison of boosters to the double vaccinated.
compared to the unvaccinated, the comp is FAR worse because case rates in the double vaxxed are far above those in the unvaxxed.
the negative VE vs unvaxxed will quite plausibly be more than double the adjusted figures above.
this was clear in the data from the UK for ages.
this is jan 6. (left) vs march 17th (right)

double vaxx had strong societal association with higher case counts before they stopped counting it and switched to only triple dosed counts.
when we compare the VE (vs unvaxxed) from each, we get this: (the red line is VE of booster vs double.)
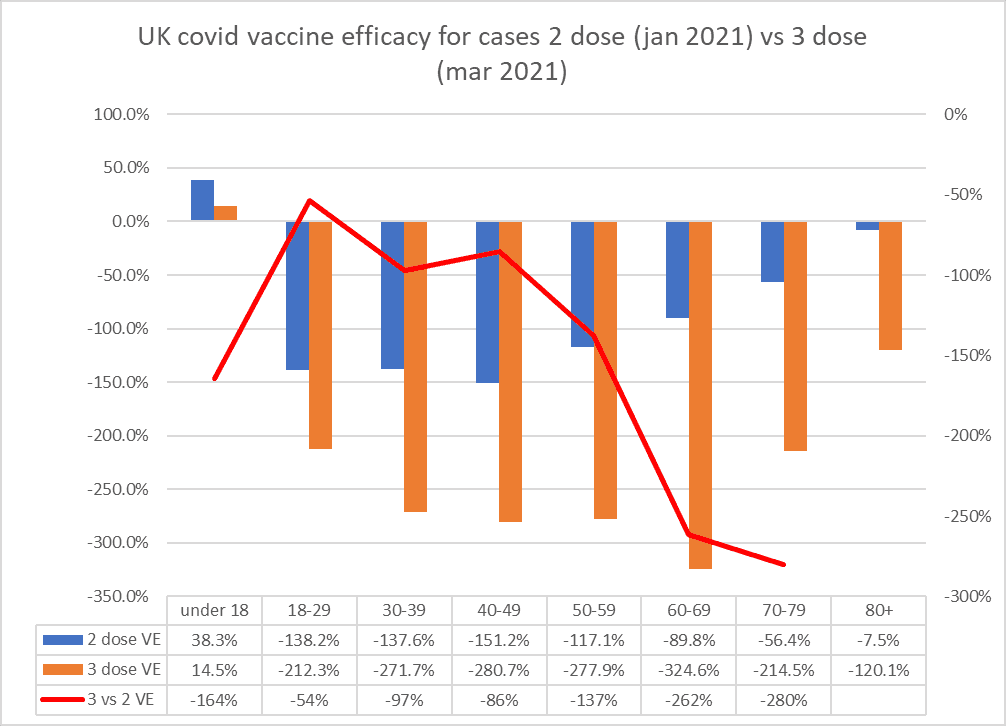
under 18 should not be trusted as it contains a massive simpson’s paradox in the age stratification and i omitted booster vs 2 dose VE for over 80 because it’s -1,493% and it makes the chart scaling wonky is is probably aberrant.
but as can be seen from this data, boosters being 50-100% risk accentuators for cases vs double dosed is well within the realm of the possible. based on UK data, it’s conservative. (or perhaps because the boosters had had so little time to fail in the israeli study or perhaps much of this is omicron vaxx evasion/OAS)
but the baseline conclusion looks pretty inescapable: the headline claim in this study that boosters were reducers of cases looks to be just data fiddling using dodgy definitions.
i mean, they proved it themselves.
but what of severe illness and death?
this has been the big claim for vaccines since their failure to stop spread became widely known.
their data here is sparser and this is the only set complete enough to work from. but it’s enough.

we can run the same process as above and get this:

which we can graph like this:
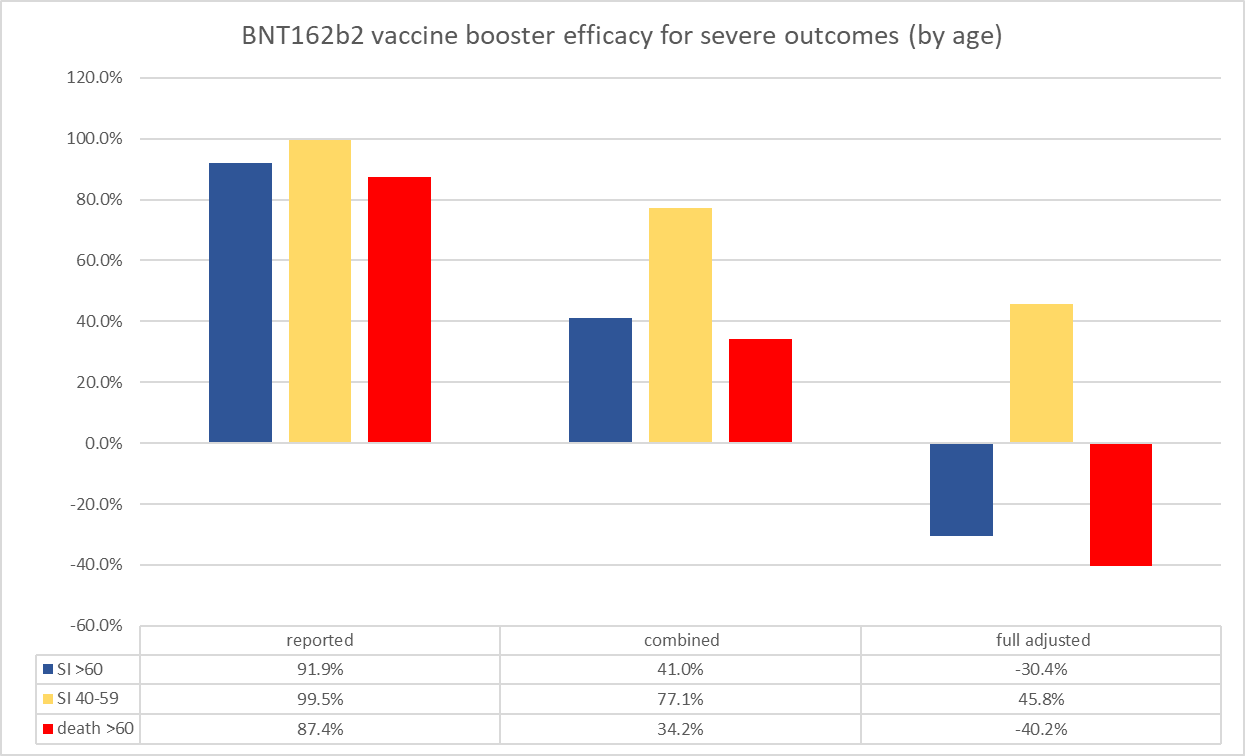
the outcomes are striking:
only in 40-59 severe illness did any positive VE remain, and that would be the demographic that boosted later and thus got more advantage from greater pre-existing immunity due to temporal shift and from boosting during disease decline vs spread period during this study interval.
so we can call that outcome a bit questionable (and we still have not worked through the potential salting of risk into the 2 dose cohort which could have further material effect to the extent that it occurred.)
another possible explanation is that the negative VE for cases looks lesser in young, so perhaps the vaccines are, to some extent, working to mitigate severity in any given case, but this protection is being swamped by the higher case counts. 30% protection against severe cases when infected but double the cases overall is still a 40% rise in severe outcomes.
differential testing rates that require more tests, esp in working age people, is another common culprit especially when any positive high Ct PCR test is a “case” or “severe case.”
also keep in mind, the israel data was pre-omicron and omicron is FAR more vaccine evading and OAS/hoskins effect enhanced than delta was, so this has likely gotten considerably worse. boosters look to be no real help on new variant antigen production.
but caveats aside, this is a smoking gun outcome.
including even a fraction of the risk window from 0-12 days post booster erases most of their purported efficacy and adjusting the figures to reflect the full risk window takes almost all of the outcomes data deeply negative vs double dosing, and this was pre-omicron.
this is definitional rigging and outright datacrime.
the bottom line is simple: you cannot trust any covid vaccine study that excludes from its outcomes those who got their dose 12-14 days prior.
treat any study using such definitions with deep skepticism.
it is not playing with an honest deck.
I have been wondering for a while how much "counting the vaxxed as those 14 days past the jab" is hurting the unvaxxed numbers. This article is shocking. It's grievous how much Pharma and govt agencies are withholding and twisting information.
I don't usually post but thank you El Gato Malo for writing all of your articles. You have done so much work and there are many of us who greatly appreciate it. And I like the cats pics. ;)
Disclaimer of Liability ™
Whilst we endeavor to make our products toxic, we make no representations or warranties of any kind, express or implied about their efficacy and safety.
We cannot guarantee that your gene 144 won’t be deleted, your X / Y Chromosome won’t be inverted, your gene 69-70 won’t be deleted or mutated, that you may experience loss-of-function due to protein folding, that your gene E1, E3, E4 won’t be deleted, that you won’t receive shots full of magnetic graphene oxides and nano-biosensors (motherboards, transistors, routers, antennas).
We do not guarantee that you won’t be MAC Addressed as per Lord Schwab’s instructions (COVID -19 is a rare but narrow window of opportunity to rethink, reinvent, reset our world).
By using our products you agree that you automatically become legally a trans-human and therefore our property since you are GM-modified using our patented mRNAs (CERTIORARI 12–398).
Trans-humans do not enjoy any human or other rights of a state and this applies worldwide. Our patents are under US jurisdiction and law, where they were registered.
Any reliance you place on our products is therefore strictly at your own risk.
...
Fact Checker: We make sh$t!
https://librti.com/page/view-video?id=1438