


will the novavax vaccine be a good booster option?
perhaps a better questions: "are any boosters a good option?" and "should we rein in this runaway train of speculative inoculation campaigns that lack sound validation?"

cliff notes:
booster campaigns have been undertaken widely in response to failing covid vaccines.
they were not supported by clinical outcomes data.
the results have been poor and seem to fail on a risk reward basis
post omicron, they make even less sense
this is the result of undue haste and insufficient testing.
therefore the idea of “faster response with novel vaccines next time” idea is one we should abandon, not embrace.
novavax has not yet been approved as a covid vaccine.
frankly, it might wind up being a safer option than the mRNA and adenovirus vaccines, but this is also a novel modality in which SARSCOV-2’s spike protein is cultured in moth cells and then injected as “nanoparticles” to induce an immune response and generate antigenic training. contrary to what many seem to think, it is not a whole virus vaccine.
it might have some better potential to generate early and possibly sterilizing immunity because it’s training to recognize actual S protein so your immune system will respond to live virus instead of to the effects of virus once it has infected cells as in mRNA vaccines.
it seems more likely to induce wider T-cell involvement. overall, at least in theory, this seems like it could be a better modality than previous vaccines, but the data as it gets out into the real world will be hard to predict. (assuming it does, a conclusion far from forgone) clearly, the output of other trials failed to map to real world outcomes and other vaccines seem to have driven rapid viral escape and selection for hoskins effect/OAS variants that not only evade but are amplified by vaccine. (because that’s what leaky vaccines do)
so, would novovax be a good booster?
i doubt it. it would probably be better than getting more mRNA, but i suspect it will fail on actual overall risk reward.
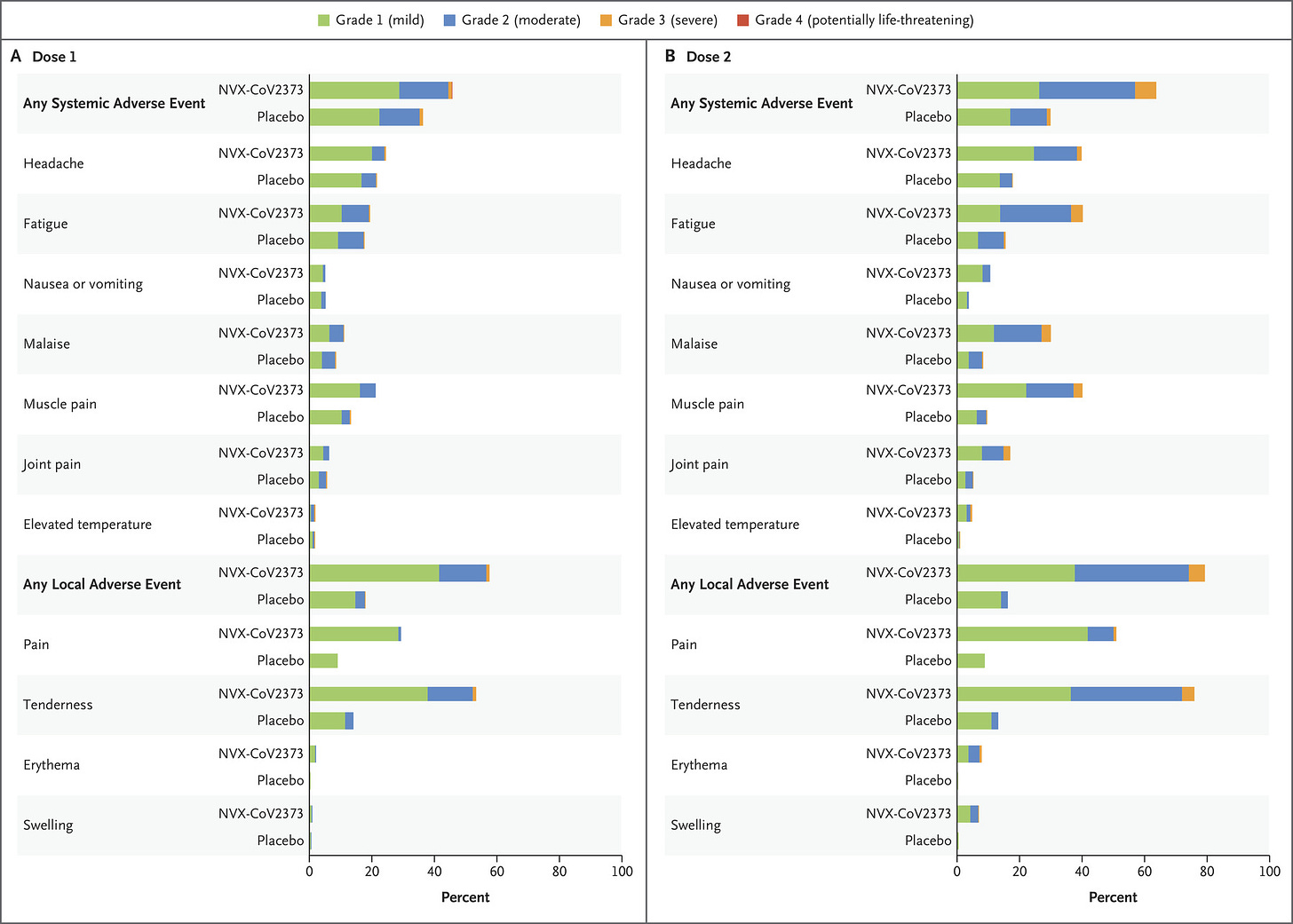
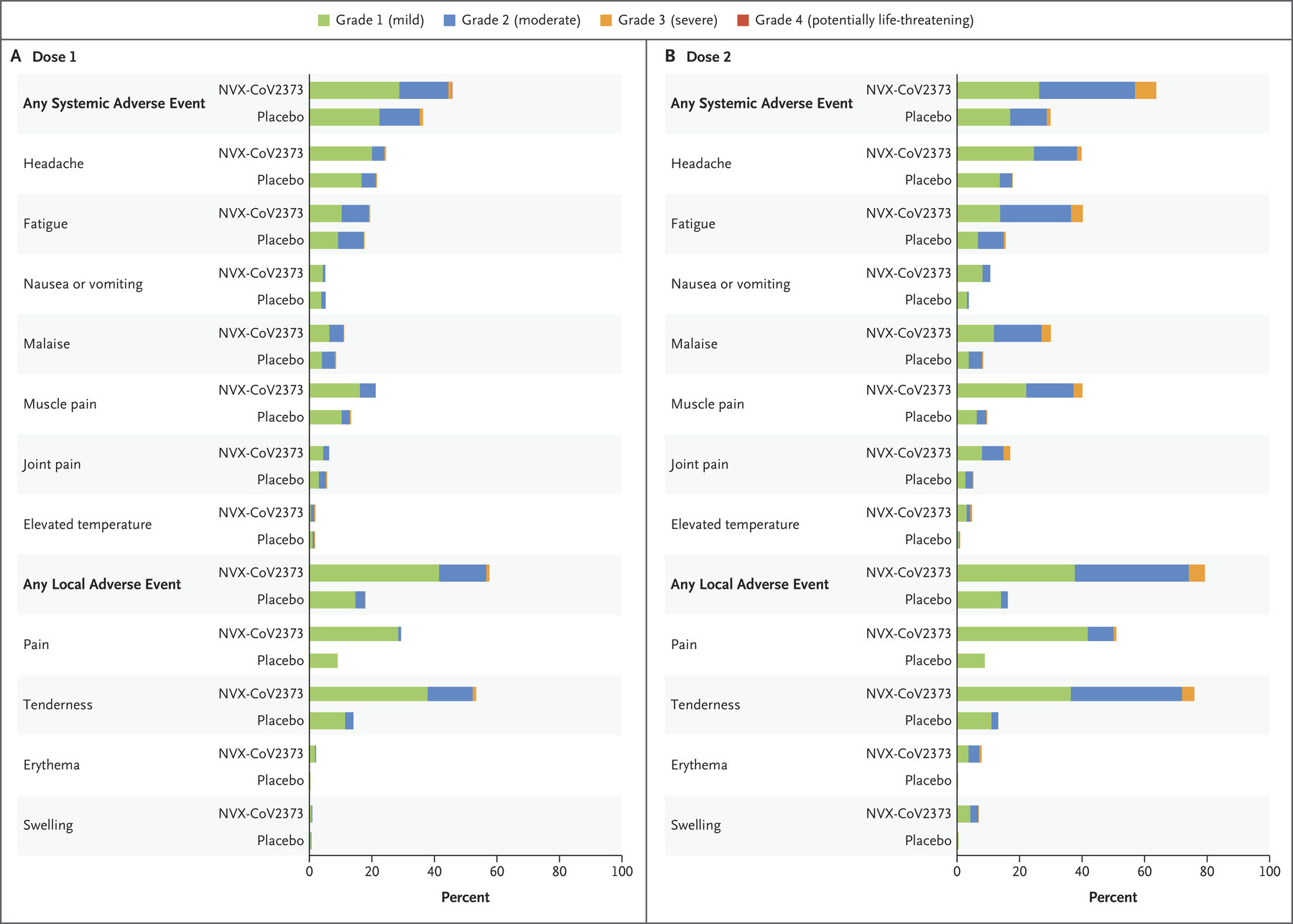
the risk is real. this spike protein is a pernicious agent and the one used in the vaccines is an older, more virulent strain. the side effect profile is meaningful and the longer term outcomes and long tail issues are not yet known. these are high levels of adverse events and i’m dubious about the level of “placebo AE’s” being this high. they also failed to screen for a lot of the potentially more worrying stuff (like clotting).
the additional effect as a booster is unknown and likely small. you’ll gain some T-cell recruitment, but whether you can overcome the antigenic fixation of the mRNA/adenovirus vaccines is an open question and whether it adds any meaningful additional protection is not known.
this vaccine will not train for N antibodies that attack the nucleocapsid of the virus. your immune system will only see the spike protein, not the whole pathogen. this narrower vector of attack makes vaccine escape easier and far more likely. there is no assurance that omicron has not already done so.
there is just not that much left to defend against. nearly everyone has been exposed to covid by now and this training to the spike protein would have little or nothing to add to the defenses of someone already recovered.
the simple fact is that with novavax we are, once more, assessing a new vaccine modality and the WSJ article, irresponsibly in my view, is making entirely speculative claims for which there is no evidence at this time.
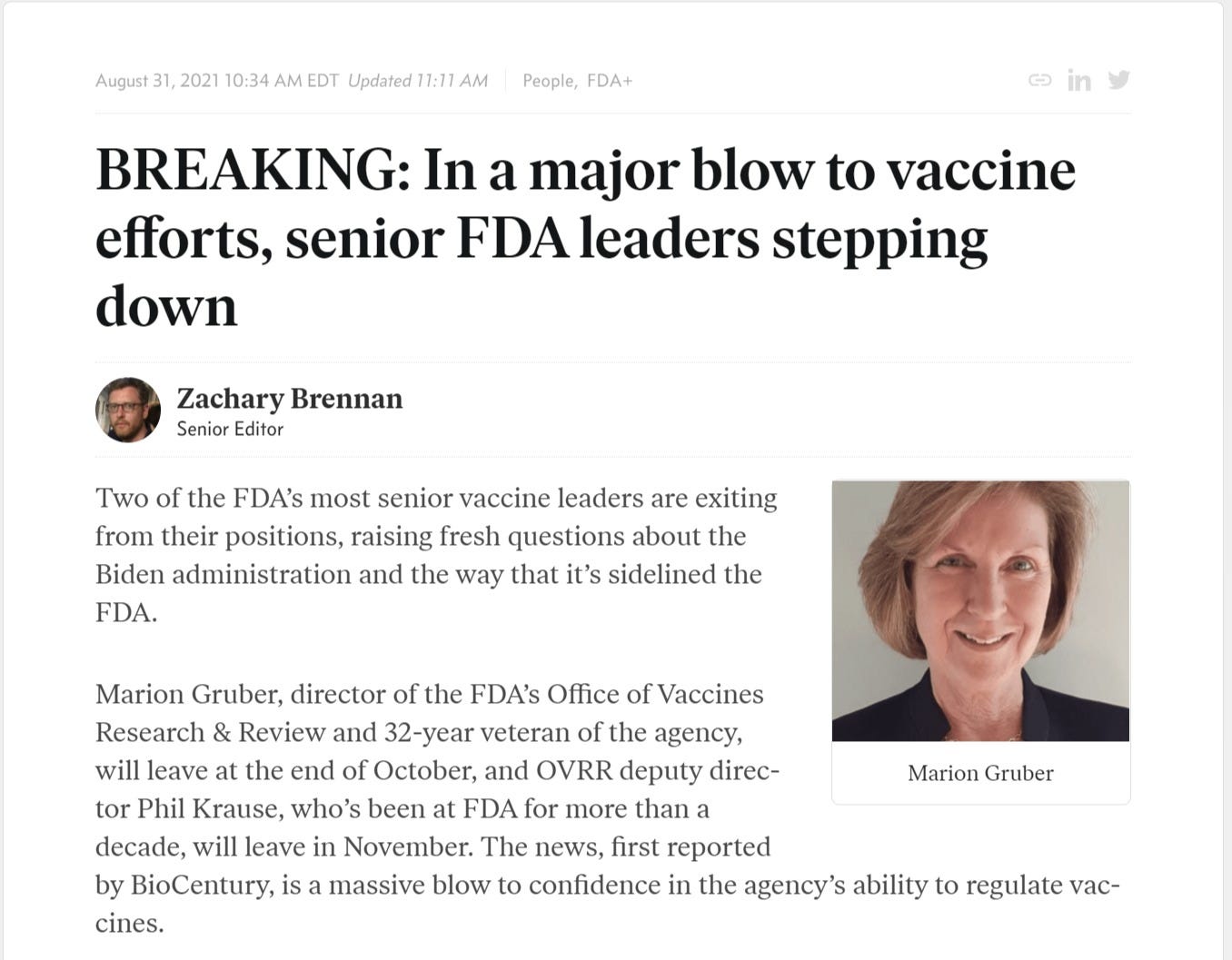
we rushed on approval a couple times already. we approved boosters based on biomarkers not clinical outcomes. corners were cut and poor study designs allowed. it has not worked out terribly well. the top people in vaccines at the FDA got so disgusted with this that they quit.
they past attempts in RSV and combo RSV flu have not panned out. this is, just like mRNA, a repurposed pathway with a string of past failures and no pre-covid successes.
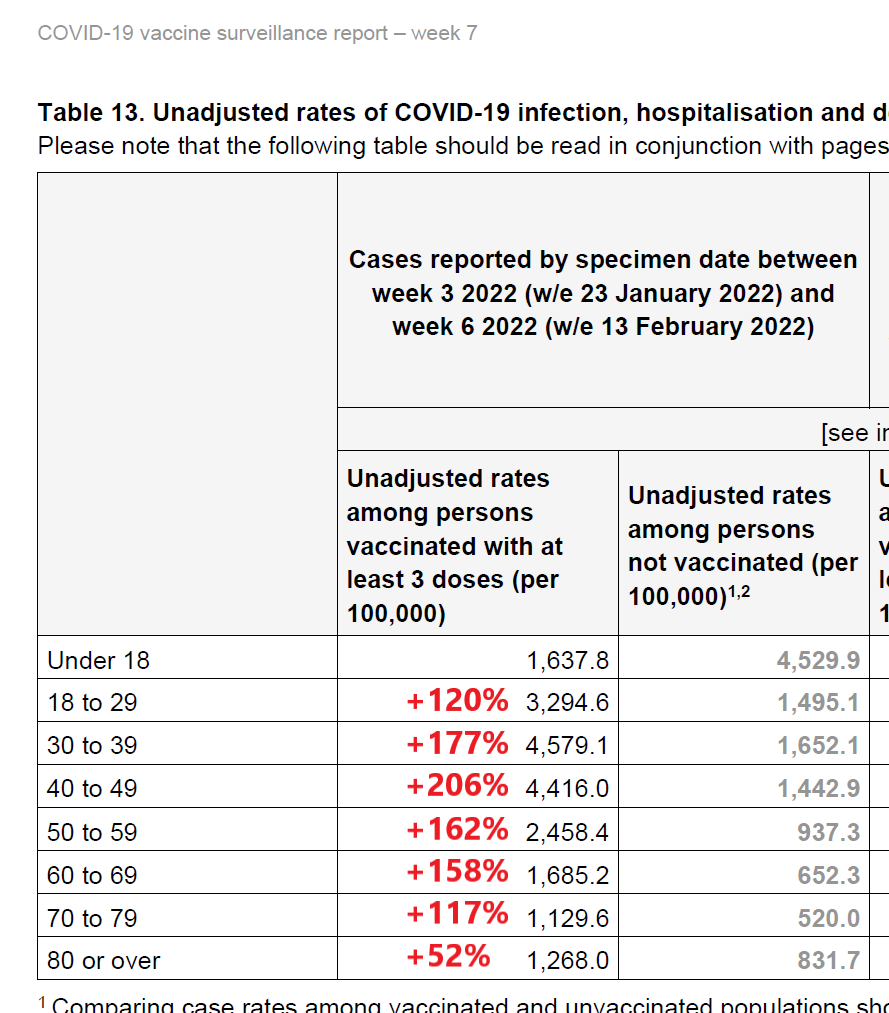
ideas that it will be a “good booster option” especially in the age of omicron look entirely speculative and the track record of “boosters” so far looks to be significantly exaggerated by the bayesian tampering of failing to count the outcomes in the vaccinated until 14 days after the final dose. on society scale, they seem ineffective and in the UK are associated with higher, not lower rates of covid contraction.
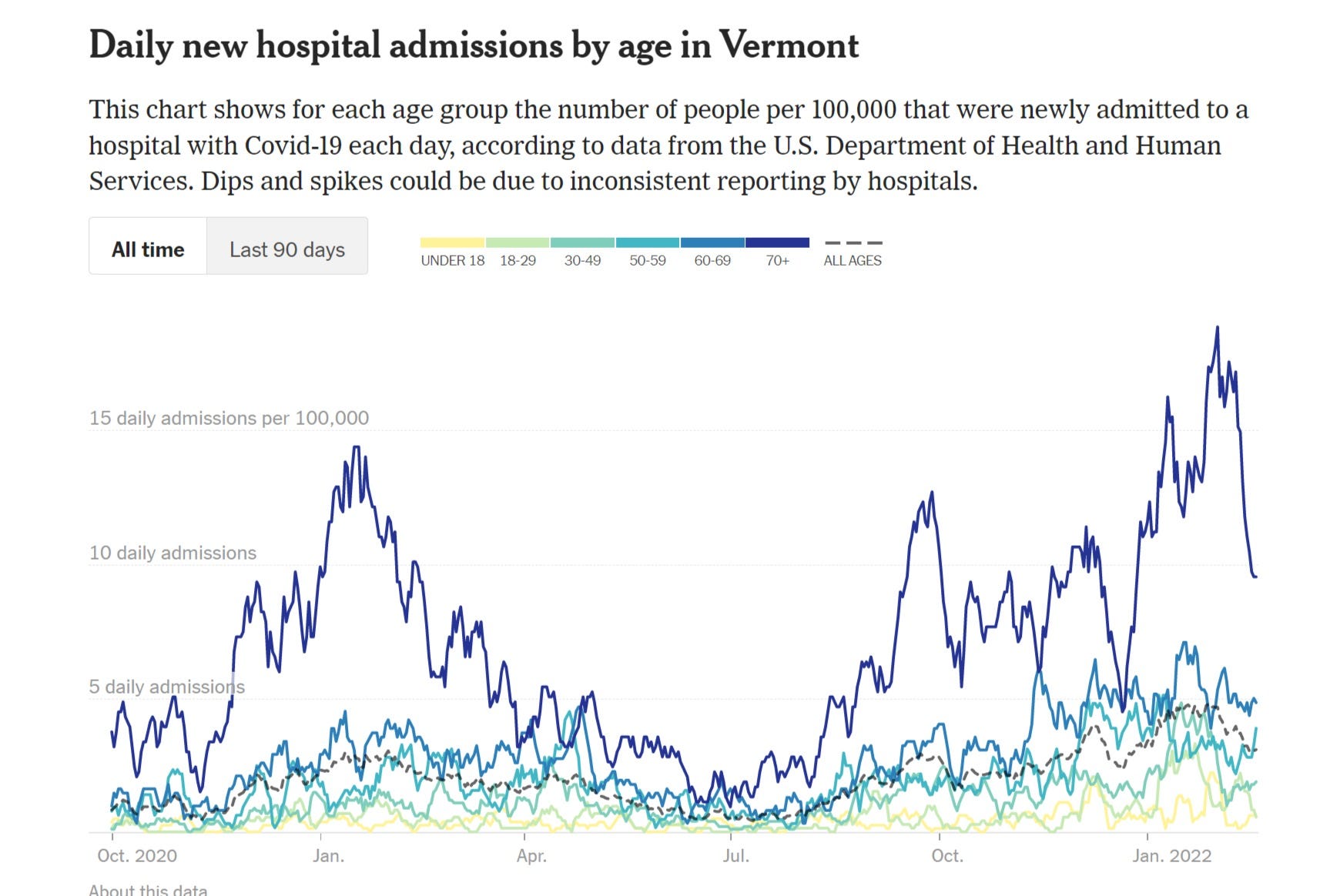
highly vaccinated and boosted groups in the US saw higher hospitalization rates this winter.
high rates of vaccination are not reducing all cause mortality. it’s actually higher, a remarkable outcome after so much cohort depletion and natural immunity generation.
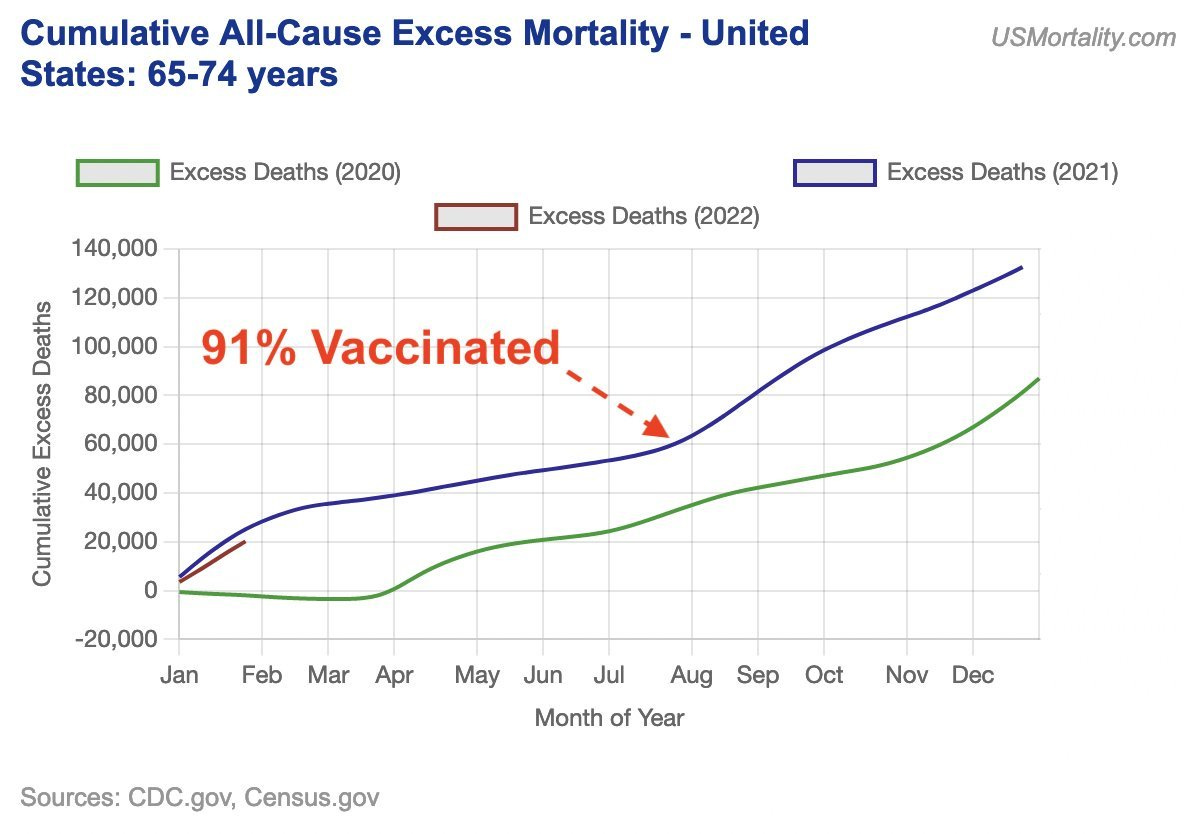
one might quibble with this chart not starting in march 2020, but even if one does, the gap to 2021 does not fully close and given the high depletion of high risk demographics, the base case would have been a drop in 2021 so exactly how to best compare this is debatable, but it looks undeniable that 2021 was higher than 2020 even if we comp april to dec vs april to dec. we’re just arguing about “by how much?”
efficacy wanes rapidly. at best, boosters are a high side effect treadmill with iffy and quite possibly no or negative benefit. (and will remain an ongoing selector for viral evolution if we keep pushing them)

but the biggest issue with the “booster” plan is that there is nothing left to protect against.
even arch-vaccinator bill gates seems to be wistfully throwing in the towel here.

omicron was a better vaccine than any made by man. (and there is a real case to be made that delta would have been had it not been driven to higher virulence by the inverted evolutionary gradient of leaky vaccines. this is how viruses have always gone endemic.)
bill seems to want to be able to move faster in the future than last time, but i suspect that one could make a persuasive cased that moving so rapidly this time is quite literally WHY we still had a covid surge this waning winter instead of having gotten past it in 2021.
you can see the resurgence of cases and deaths in a gompertz violating double hump pattern in places all over the world. it coincides with vaccine rollouts and aligns with known immuno-suppressive and longer time susceptibility amplification data.
speed is not a virtue in vaccines, efficacy is.
therefore, it pays to take your time.

well we needed something!
no, we didn’t.
leaky vaccines are worse than no vaccines at all. they drive worse long term and societal effects. they can be very, very dangerous.
ask a chicken about marek’s disease some time…
vaccines have traditionally been trusted and safe because we spent 5-10 years testing them before rolling them out and pulled them off the market for adverse events profiles orders of magnitude lower than what we’re currently tolerating.
we pulled the swine flu vaccine for fewer than 100 cases of guillian-barre syndrome from the vaccination of 25% of US population.
today, THIS is being called safe.
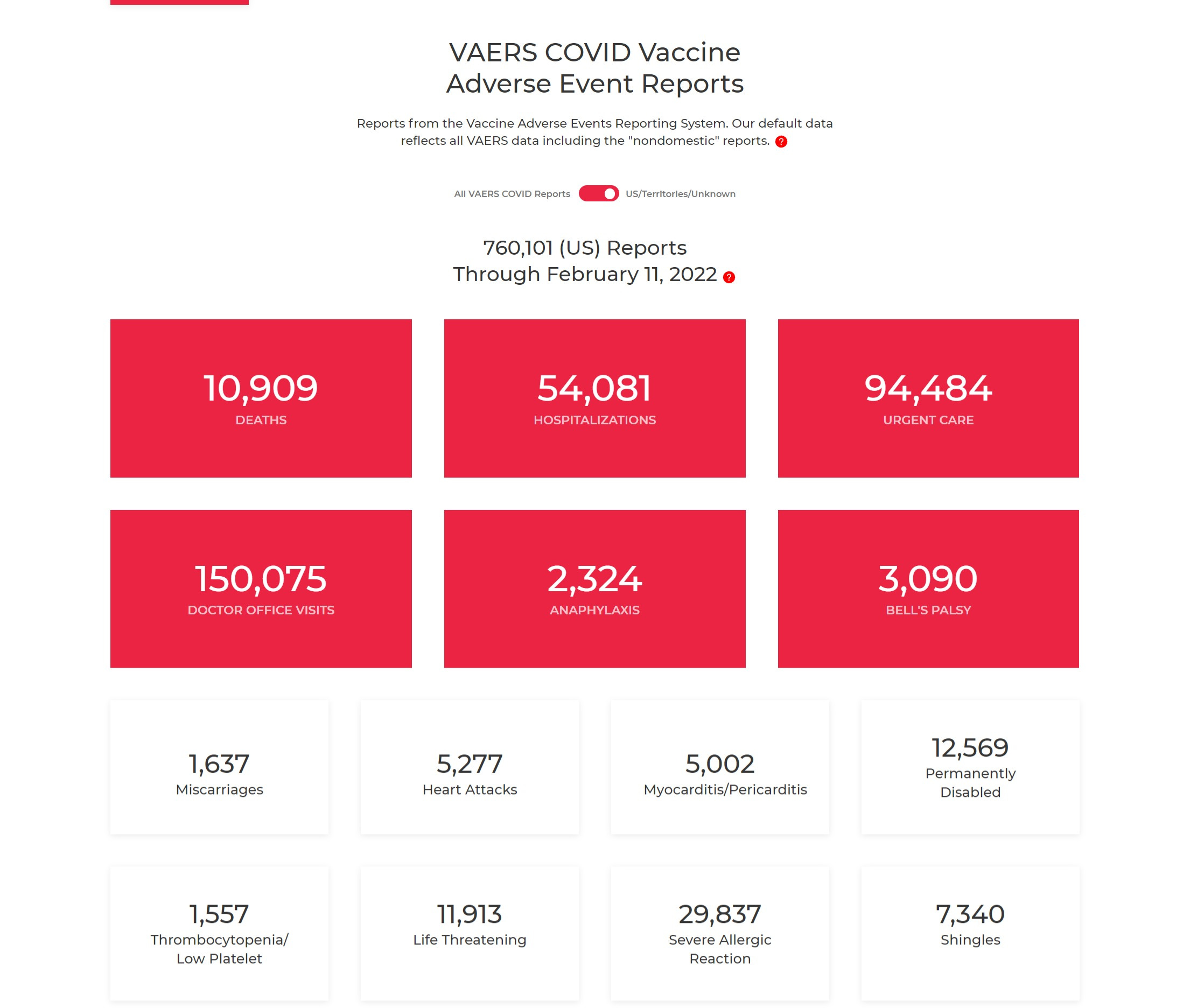
VAERS likely undercounts by 90%+ so these numbers are just intended as a sort of tripwire warning.
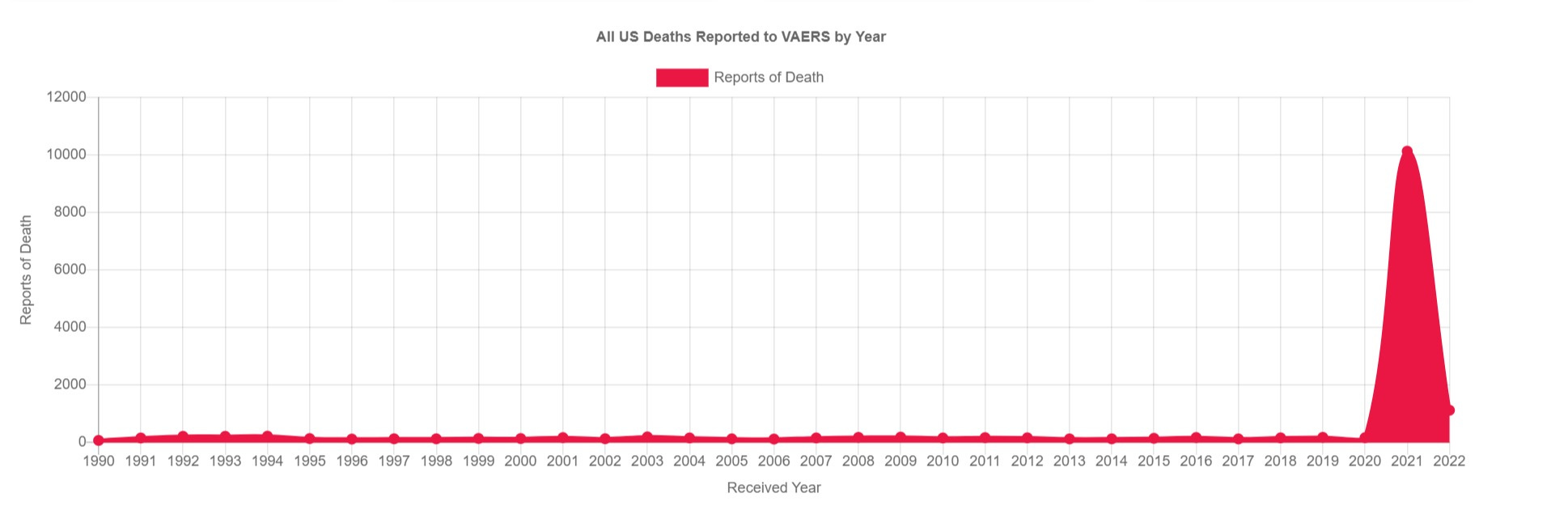
but if this does not set off the alarm, i am honestly perplexed as to why we bother having this.
and israeli data on booster AE’s looks grim. this (quite new from the looks of it) substack takes a great tour through the data.

maybe rushing these assumptively founded and outright presumptive interventions and new modalities to market is not such a great idea after all…
things are sure not going better in israel as a result.
the evidence here is pretty overwhelming:
this gatesian claim that we need to push vaccines faster for “next time” is a very dangerous idea and one we really need to abandon.
it is not good practice and the outcomes will not be better next time.
another round of “play stupid games win stupid prizes” may be great for pharma profits and NGO powerplays, but it is not a sound basis for public health.

i'll never take any vaccine ever again i dont care if its made of fucking rainbows
Bill Gates comment “Sadly Omicron is a better vaccine” what the actual F$ck