


if boosters stop the spread of covid, why don't we see it in the data?
a look at highly boosted denmark and iceland

prior to now, getting vaccinated in the middle of peak disease season was generally not recommended. you did it before, not during. this is because immunizations stress your immune system by provoking it into a response. this is not a great strategy during times of high active risk.
yet, in another of the seemingly endless inversions of policy from “what we always did before” to “aggressive interventions of dubious efficacy pushed with great certainty despite a paucity of evidentiary basis” it’s suddenly “just common sense” that we need boosters during peak season to stop the spread.
there is not actually any good clinical or societal scale data to support this.
at best, it’s iffy biomarker studies on antibody levels being peddled as a fix for what now looks pretty conclusively to be very rapidly declining covid vaccine efficacy over time and the seeming flip to negative efficacy against cases.
thus, it is argued, we need boosters to reverse this trend.
so, i looked at a couple of highly boosted countries so see how that policy has been working out.
(all data from our world in data)
first, i took the cases counts and normalized them to current testing levels to try to remove the effects of big changes in sampling rate from the actual epidemiological signal.
i then plotted cases in 2021 vs 2020 and overlaid it on top of the boosted rates in each country.
if boosters were stopping or slowing spread, you’d expect to see their rise in prevalence start to bend the cases curves. but we do not see this. this leads me to doubt that they are having much or perhaps any positive effect. one can have correlation without causality, but having a large causal effect and failing to correlate to outcomes is pretty implausible. both look pretty much the same as the lower boosted neighbors (like finland)
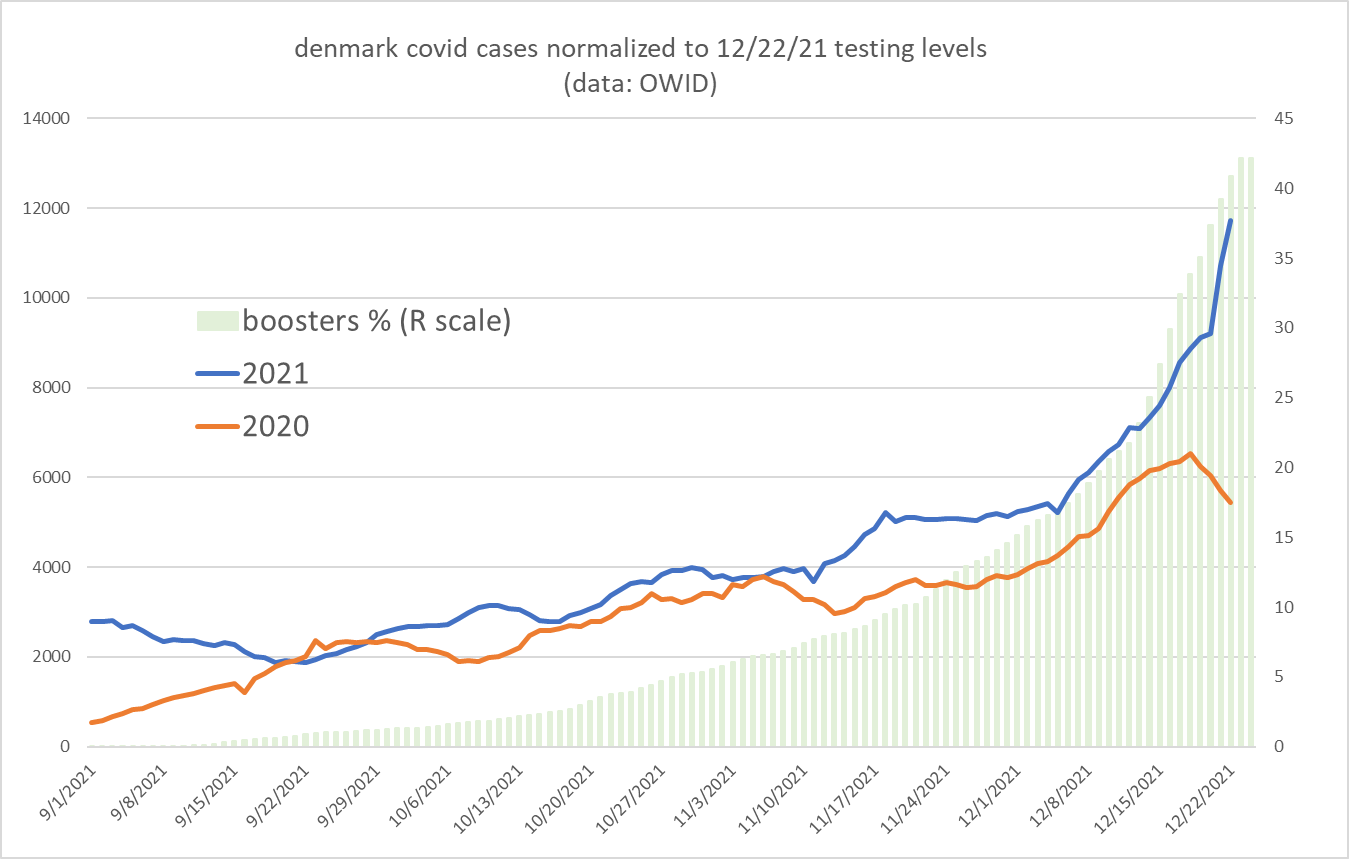
coming into mid november, covid cases in denmark looked very similar to 2020. (despite greater natural immunity and a societal vaxx rate in excess of 80%) boosters really started to take off in december rising from 15% of the population to 42% as of 11/24. this has clearly not reduced the case rate or lessened its slope.
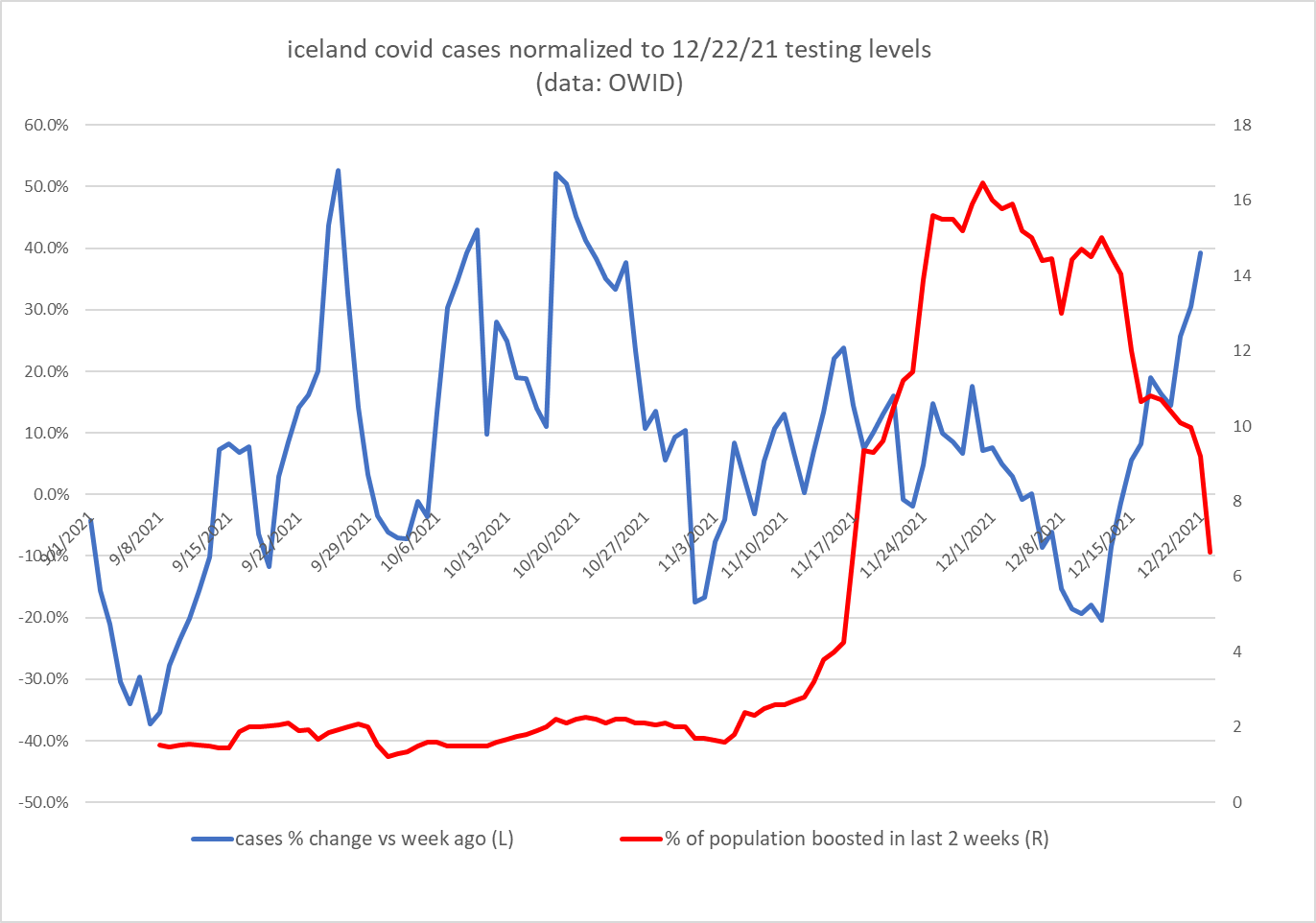
this is even starker in iceland who is also over 80% vaxxed and nearing 60% boosted (perhaps because iceland seems to have had less covid overall)

one could perhaps more plausibly argue that boosters have correlated to a rise in cases but we’re getting onto thinner ice there as the correlation could run the other way (cases are driving people to seek boosters) or the two could be unrelated and the rise is simply variant driven and booster rate exogenous. i’m not sure exactly what we can prove here in that regard at this point from this data (perhaps nothing) but there are some quite provocative alignments.
i generated two series of data:
the change in testing normalized case counts vs 1 week earlier
the percentage of the population that has received a booster shot in the prior 2 weeks (the period that many studies have shown to be associated with immunosuppression/higher incidence of covid cases post covid vaccination)
thus, we are not randomly mining for data but looking for correspondence in variables we have a strong, a priori reason to suspect are linked and causal.
it yields this:
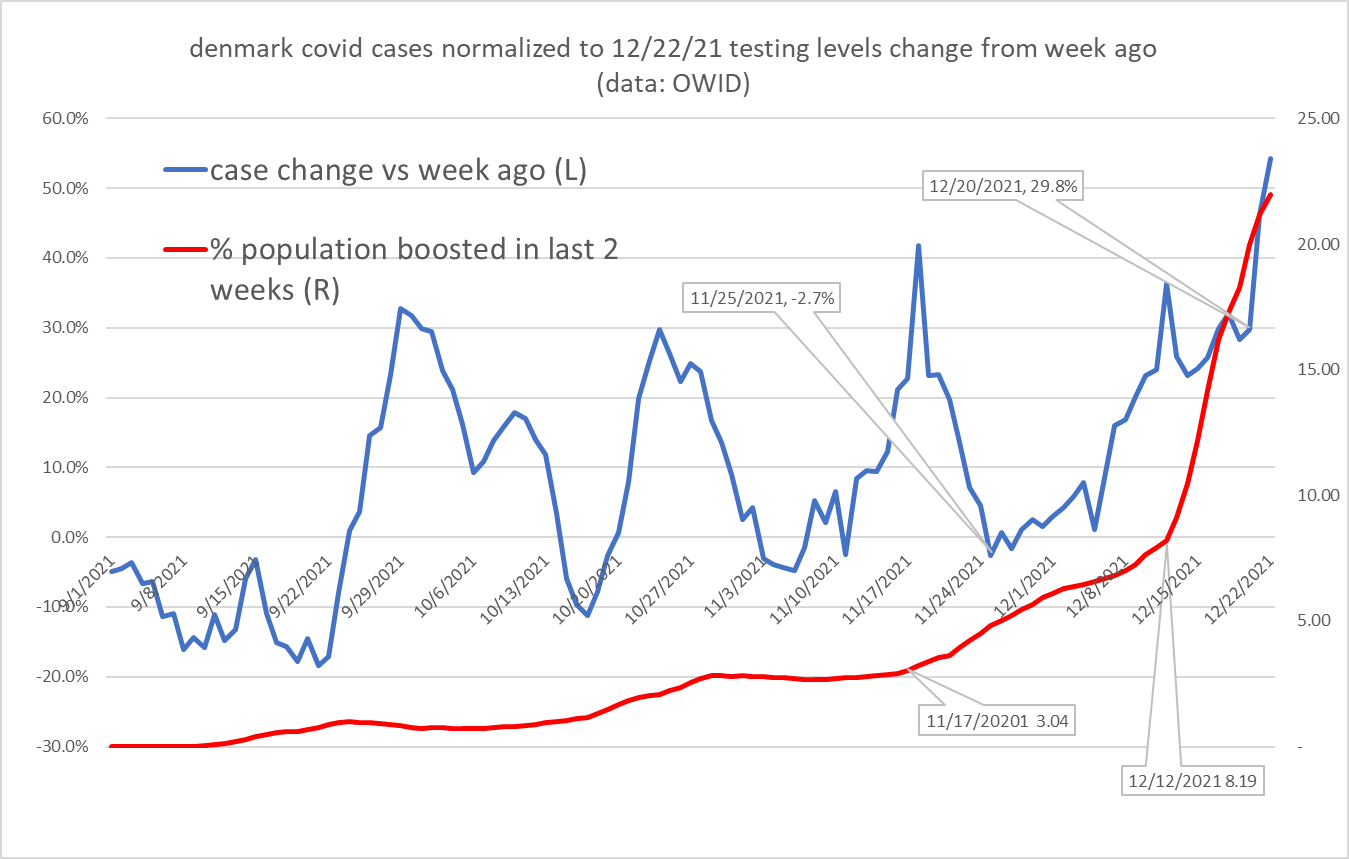
inflections in the size of this risk cohort seem to be followed ~8 days later by inflections in the rate of change in cases.
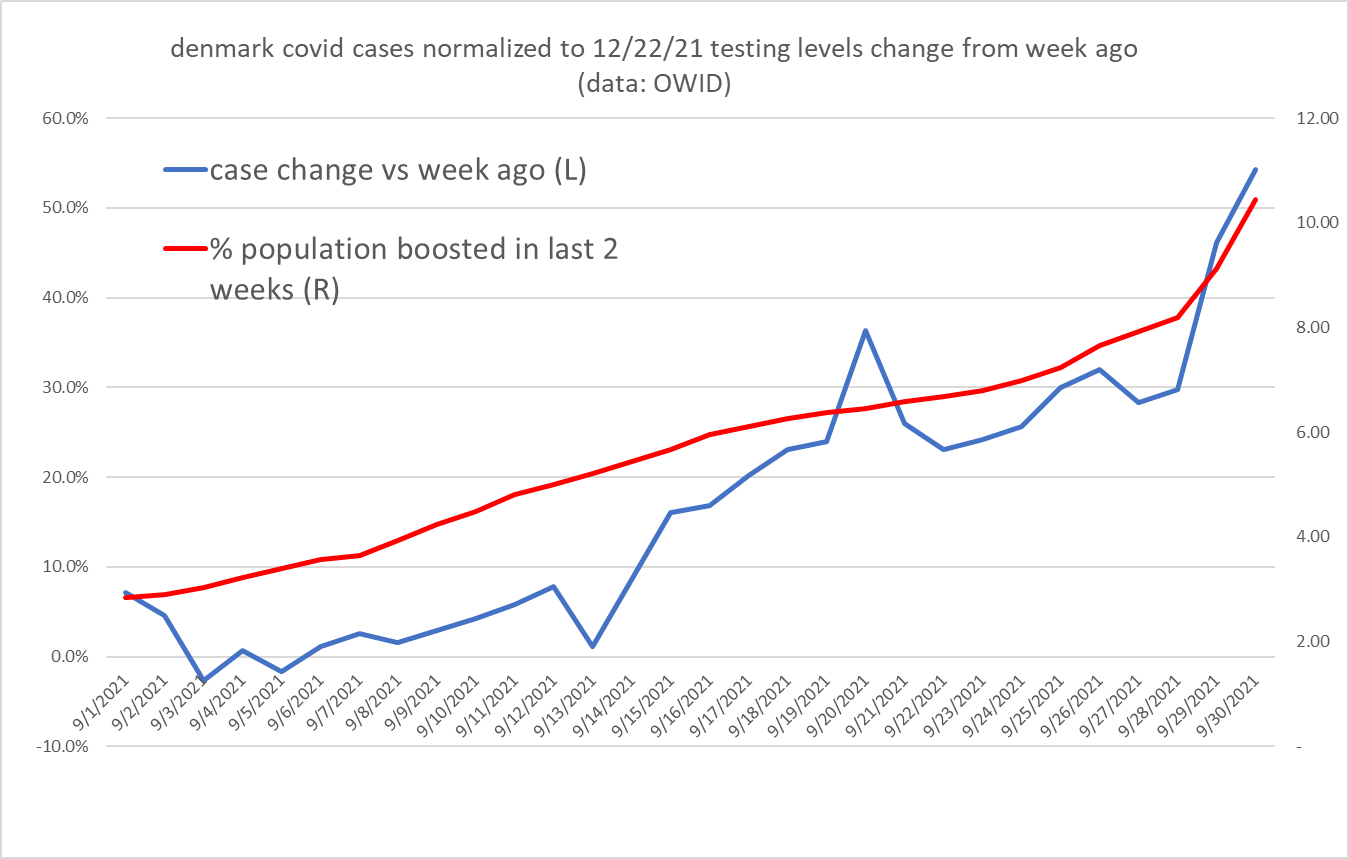
not dispositive but certainly provocative, especially if we zoom in and shift the pop data 8 days to overlay what could be cause and effect:
as tantalizing as this is, the same effect seems totally absent from the icelandic data. this may well mean we’re just chasing ephemera and seeing patterns where none exist.
several possible explanations occur to me:
this danish correlation is spurious/meaningless
this is driven by a variance in which vaccines are being used
there is some other confounding factor
i’m not sure we can rule any of them out at this point.
with regard to point 2: it’s really only known that this worry window of immune suppression is driven by the mRNA vaccines.
denmark is heavy on mRNA having barred both JnJ and astra zeneca from use.
iceland has used both the AZ and the JnJ vaccines widely. novovax is also approved for use there.
i lack any good data on what is being used as boosters and on top of what previous inoculant they are being applied in the two places and if someone has it, this might be illuminating in terms of helping to assess this seeming variance in outcomes/relationships.
it has long struck me as odd how little data there seems to be on any sort of societal scale on this.
we lump “vaccinated” into one big category despite there being several quite different vaccines using quite different modalities. it seems reasonable to expect that their efficacy and side effects might vary considerably. why this is not being tracked and reported is a puzzle. this would seem like an incredibly important salient to guide medical choice and a glaring lapse in the collection and dissemination of useful medical data.
to sum up:
i think we can say with fairly high confidence that there is nothing in this data that supports the idea that widespread booster usage is stopping spread or contagion of covid.
the issue of whether they are, in fact, making spread worse remains open and the data seems mixed and wants for greater explanation, though several studies seem to show negative vaccine efficacy for boosters on case counts (link below), so i have a hunch there may be something to the notion and will keep scratching at it.
Even my boosted friends no longer argue that it has any effect on stopping infection, likely because they're all sick right now. However, they're still clinging to the "less sick than we would be" argument, and I can't really blame them, because the side effects they experienced with the shots were pretty crappy and they need to have something to show for it besides subclinical heart damage and messed up periods.
My 28 year old healthy and skinny Nephew got three shots in 8 months. His booster was last Saturday and he was in bed, knocked on his butt. By Monday he felt better only to be sick on Wednesday and tested positive for COVID. Now imagine being a healthy 28 year old who has almost zero risk of hospitalization from the RONA, assuming all the longterm risk of MRNA and still getting the virus. If that is not a terrible outcome for humanity and yet it has happend all across the globe. Why would we expect people to think prior to getting the booster when they did not think, do their own homework, research and understand their true risk profile prior to starting their COVID sacramental jabs???