


testable hypotheses on BA.4 and BA.5 covid variants
are they causing death spikes in the vaxxed/boosted?


that which cannot be falsified cannot be proven.
this is a simple scientific tenet and a core of the scientific method. one must always strive to disprove hypotheses. it’s the only way to know if you can trust them.
so let’s see if we can lay out some standards by which to do so here:
omicron appears to be evolving into variants and sub variants more rapidly than past covid strains.
this could be for a variety of reasons including chance and vaccine driven homogeneous herd level antigenic fixation with non-sterilizing response which would create both a readily infectible substrate and a perfect breeding ground for strains to seek advantage in infection.
mostly, the evolutionary gradient will push a virus to be less lethal. killing the host is maladaptive to the directive of the selfish gene: make a copy of me and pass it on.
wiping out your home and your travel vector is not a survival and spread optimizer.
but “mostly” is a tough thing to bet on over time when you’re rolling so many dice over and over. sometimes, you get aberrations and optimizations and if the herd has highly homogeneous immunity from leaky vaccination campaigns you can get vaccine accelerated spread as seems to have already been prevalent but also might at some point roll snake eyes and trigger deaths.
there is a thesis going around that the BA.4/BA5 variants are such a roll.
the basic premise is this:
this variant became prevalent in south africa and then later portugal. (these 2 seem to be leading for some reason that is unclear to me)
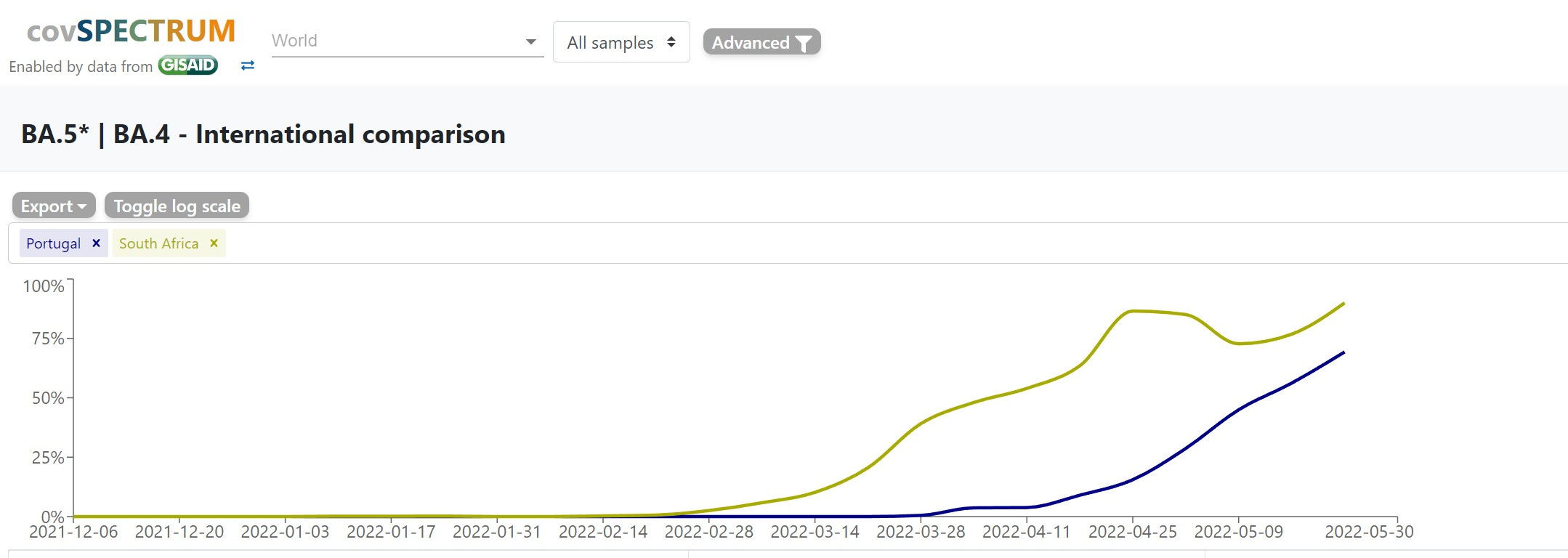
this has led to a spike in deaths in portugal, but not in south africa.

the two countries have very different vaxx and boost rates.
SA is 31% vaxxed, 5% boosted. portugal is 87% and 64%. (using OWID data that seems to be a bit behind for portugal)
the hypothesis is that the variance is down to vaccines. (but, obviously, it could be a lot of things)
gatopal™ igor lays out the notions in detail here:

whether or not this is true carries major implications about what’s coming. the US has seen basically no BA5 yet, but just passed 5% of cases the week of may 23 and this strain tends to take over once it gets going.
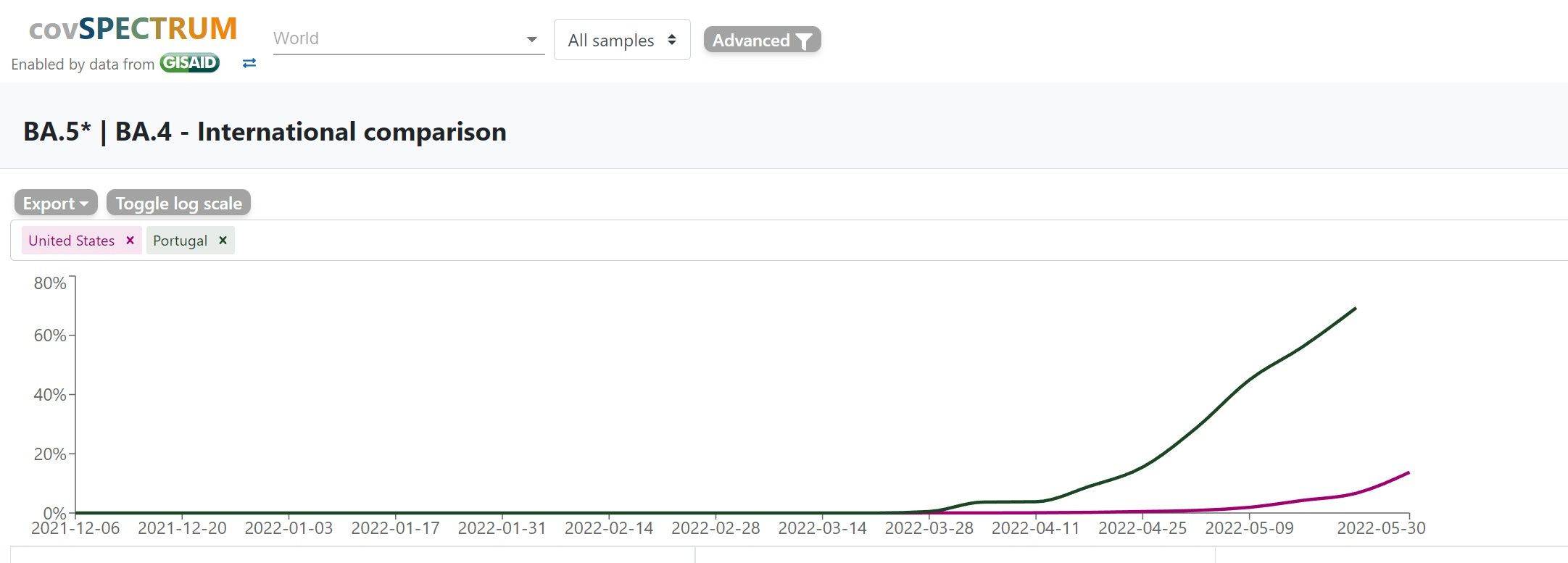
are we going to see deaths in the boosted rise rapidly (as hospitalizations did last wave) or is portugal some sort of aberration?
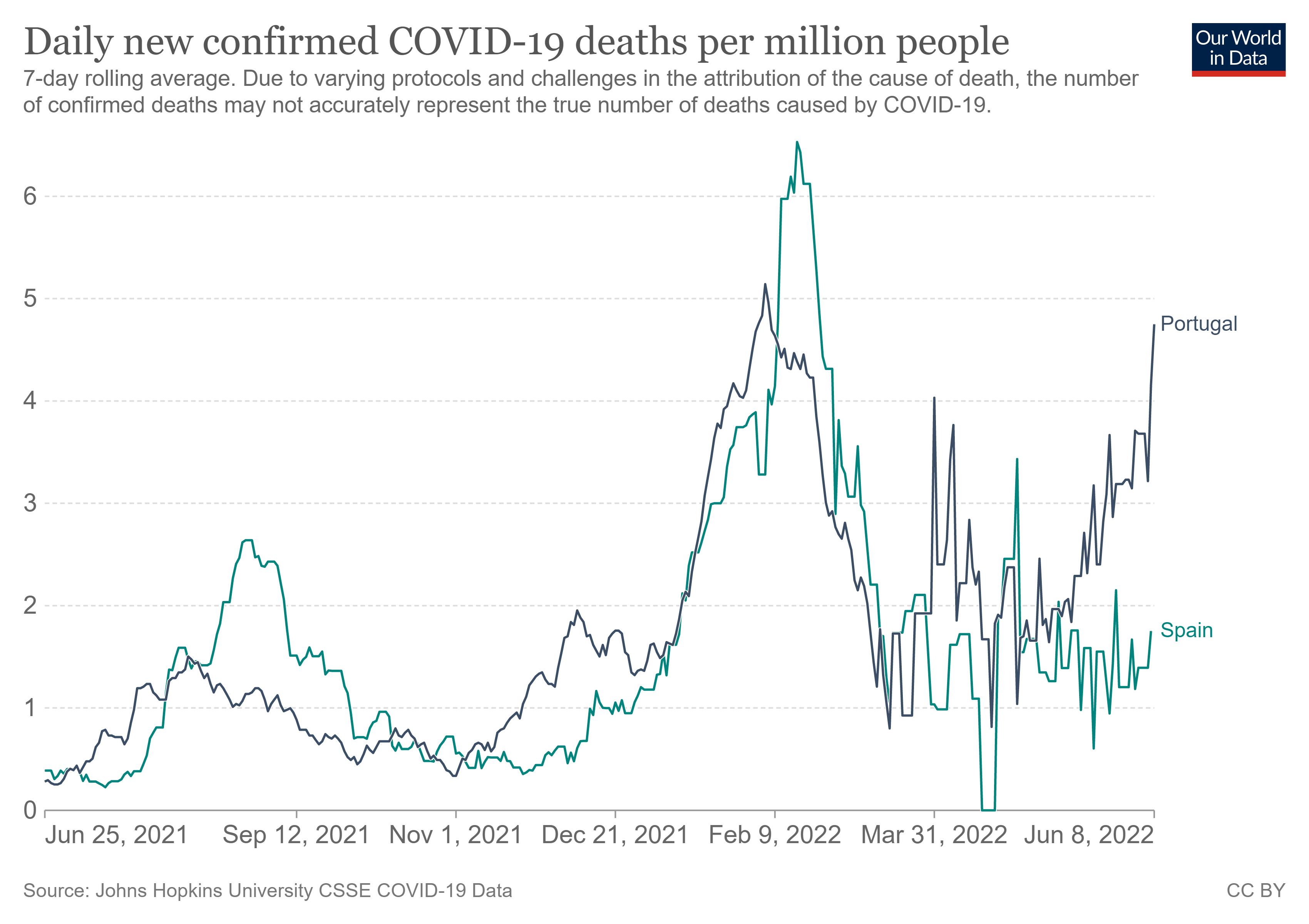
they key to this puzzle looks like it might be spain. they will be the canary in the coal mine.
the iberians have had very similar covid experiences, tracking one another well and ending up near identical overall with 2317 (portugal) and 2285 (spain) deaths per million population.
but since may 9th when they were all but identical in deaths per mm per day, they have diverged strongly.
and so too did BA4-5 prevalence.
but it is now rapidly converging. neighbors tend to rapidly share variants.
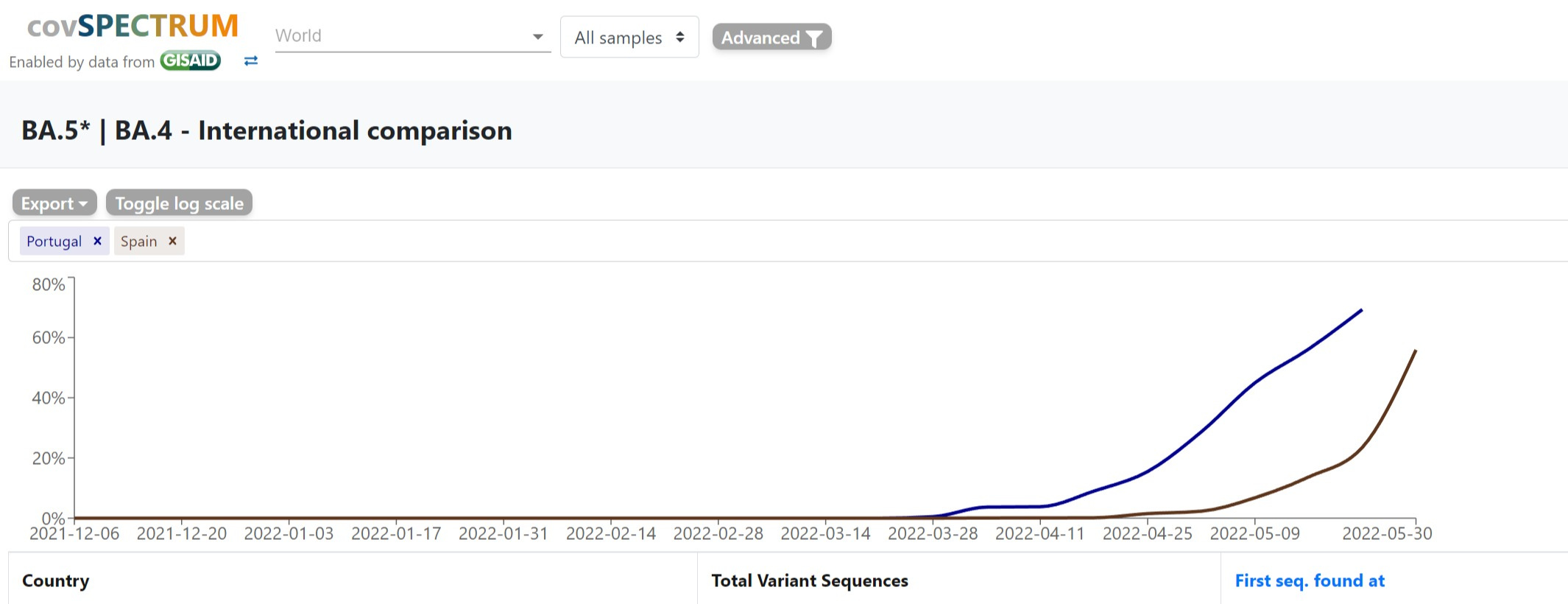
it was about a month from when portugal started to ramp up in earnest on BA4-5 to when deaths began to rise.
it has now been about a month in spain since their variant ramp began.
this means that their deaths count over the next couple weeks is going to be highly telling.
their vaxx and boost rates are similar to portugal. (87% vaxxed, 54% boosted)
if it spikes like portugal, then the vaccine enabled thesis (while not proven) remains intact.
but if it does not, it poses real problems for this theory and makes one suspect that portugal may be some sort of outlier and/or that BA4-5 is not especially dangerous and has conformed to “most” evo gradients and continued the path of attenuation to endemic (like other common cold coronaviruses).
this sets a sort of natural experiment.
you make predictions, set falsification criteria, and you see how a hypothesis holds up.
and so we wait. and we watch.
we should know quite a bit more in a couple weeks.

(one possible confound could be a variance in vaccine types used in spain and portugal. i have no real data these and continue to be amazed at how poorly this is tracked and aggregated. if anyone has a good source for global data on that by country, i’d love to see it)
A great idea that you have, to test more -- as many as possible -- countries that are similar in some ways, but different in others. I would absolutely LOOOOOVE to know the outcome! It would be great to even somehow automate that.
Also Ba5 is rising in the UK and hospitalizations are rising disturbingly faster than cases. (cases in UK are meaningless due to ending of free testing)
…but Jan 6th