
do first vaccination shots increase spread and covid deaths?
a look at palestine

in THIS analysis, i was using palestine as a control group for israel because their vaccination rate is about 10% vs 60%+.
but gatopal™ ben @USMortality pointed out something interesting to me. palestine just started a big vaccination push that did not show up in my data because so many folks have only had one dose so far. useful data. it’s good to have pals!
we can see this here:
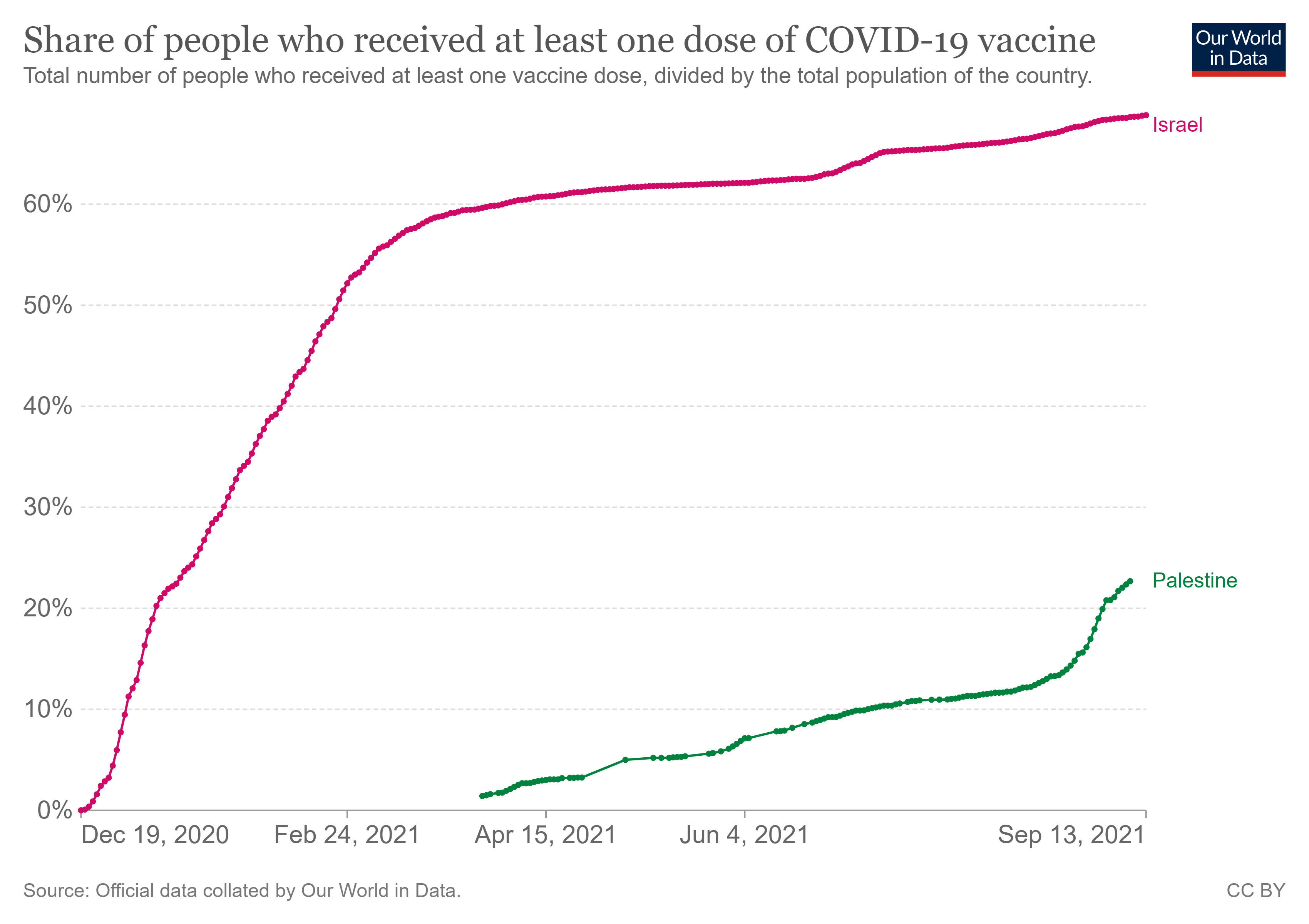
this sudden rise provides an interesting test case for the “are vaccines causing disease spikes” hypothesis. (it also makes palestine less useful as an unvaxxed control group for israel)
so i plotted this rise in vaccinations per day vs the palestinian death rate.
the results are provocative.
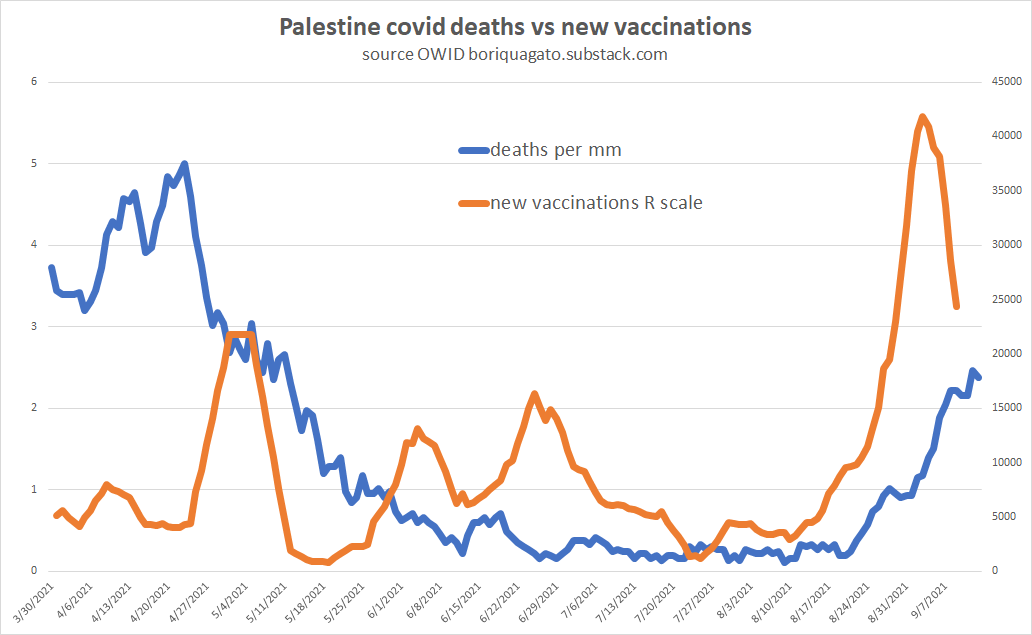
we see first doses pick up, then, about 14 days later, deaths follow suit. like israel, we have possible seasonal confound, but we also see exactly what we would expect to see if vaccines were weakening immune systems and accelerating spread and/or enhancing death risk.
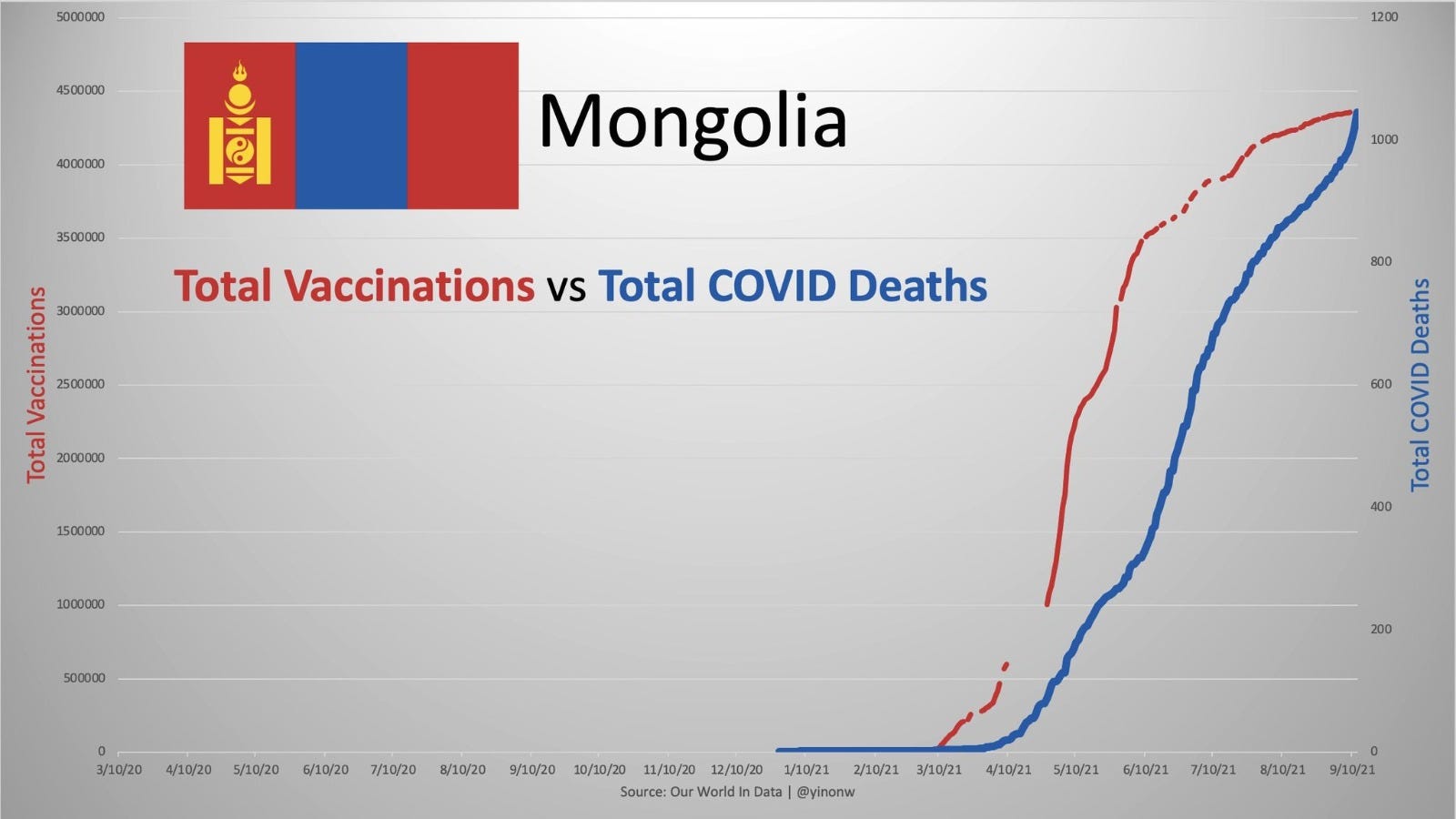
and wow does this look more than a little like mongolia.
that said, we also saw this death rate fail to spike on the vaxx push from may to july. this lack of correlation in the spring/summer requires explanation if we’re to persist in the hypothesis that vaccines are driving infections and deaths.
my current working theory on that is rooted in risk amplification.
if, as this STUDY shows, vaccines have a negative VE in the two weeks following initial dose, to measure the impact, we also need to see the size of what’s being affected.
at a time of low seasonal disease prevalence a doubling of risk might be negligible. 2X 0.01% = 0.02% and you barely notice. you get swamped by the declining trend. it’s like doubling the risk of getting eaten by a shark while you’re in your living room.
BUT, if we double the risk at a time of HIGH seasonal prevalence, a doubling may be a big deal. 2% becomes 4% and suddenly you really notice. now you’ve doubled your shark risk during shark week on the great barrier reef. and THAT is a different kettle of fish altogether…
this seems to fit with past seasonal patterns and looks promising as an explanation.
as an interesting check, i went back and looked at the original israeli data from december 2020 to may 2021 when their first doses were being administered. this too is provocative and just like the recent data, it seems to show almost no lag on vaccination moving to deaths. (note that i have switched to “new vaccinations” from “% vaccinated” because it’s a more useful number and avoids autocorrelation issues going forward.
the 2 sided correlation is remarkable.
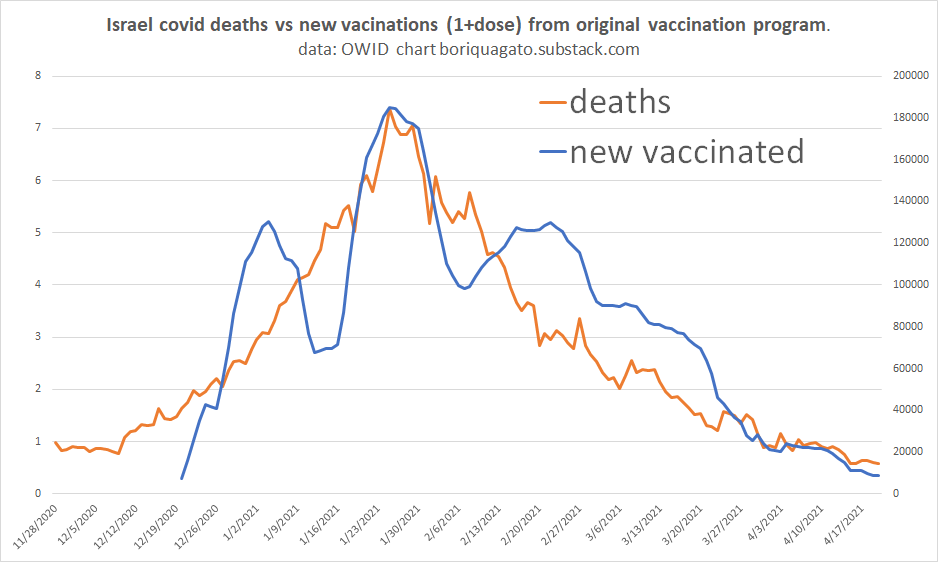
so, more pieces come together and we’re seeing more likelihood that vaccines drive deaths for a period post dosing. one could argue that the israeli data is consistent with deaths making people run and go get vaccinated, but the lags of deaths post vaccination in the palestinian and mongolian data pose problems for that theory on direction of causality.
this could also be coincidence, but as more data piles up, that will get harder and harder to claim.
it seems the next step will be to test some other cases by looking at countries that had big vaccine pushes during peak covid and some others that did so in periods of low seasonal risk/decline.
that should help us round out this theory and see if it holds any real water. the real test is always to make forward predictions and see if they hold.
so, for rigor’s sake, let’s lay out a specific hypothesis:
vaccines produce a 14-21 day window of increased risk post administration.
this is evidenced by a rising death date 0-21 days post vaccine adoption and proportional to it.
the death rate will also be a function of the seasonal risk level in any given region.
SO: if we find many places with deaths rapidly following vaccines administered in periods of high seasonal risk, it will bolster this theory.
finding examples of vaccine administration during such periods that had little or no acceleration effect despite peak risk would weaken the theory.
OK.
time to go look for data. if anyone has any for either side, let me know.
Thank God there are people (cats) such as you with explanatory skills willing to engage the data and be transparent enough to invite other experts to participate in your discussions and share data etc. In a sane world wouldn’t we have, like a weekly covid round table panel once a week and it would be on tv and the best scientists, experts, and reporters and cats could share their best thinking and their best questions in transparent fashion, publicly? Kind of the opposite of the way public health information is being handled. Keep up your important work and thank you.
Tweets like these make me wonder if it's vax injury:
https://twitter.com/AxelSavage4/status/1437624425281511429
https://twitter.com/Zieleds/status/1437752904811646981
@AxelSavage4
Sep 13
3) Apparently all patients are asked whether or not they received the #CV19 vax, no matter what issue it is that brought them into the ER.
If the patient received the vax less than 14 days prior, they are recorded as "Un-Vaxxed"
4) The story the nurses are being given, is that this is done because the vax takes 14 days to start working. The FT ER nurse my wife talked to last night has a different theory:
5) It has been her observation that most patients coming in with what appears to be vaccine injuries are coming in within 72 hours of receiving the jab. By recording these patients as "Un-Vaxxed" they can do a few things:
6)
- one, they can claim those vax injuries are a result of Covid & not the shot
- two, they can bury the vaccine injury
- three, they get to claim there's a "pandemic of the unvaccinated"