


the long and short of "long covid"
PASC me no questions, i'll tell you no lies

this STUDY performed at NIH in bethesda sheds yet more light on the purported symptomatic and clinical expression of what people are terming “long covid.” they refer to it as PASC (post-acute sequelae of covid) and therefore so will i as we discuss.
first, some priors to keep in mind: there is such a thing as “long everything.” virtually every disease and clinical condition from flu to cold to pneumonia, broken bones, or severe traumatic stress can cause lasting effects, some quite severe. flu can and does cause permanent neurological damage in some people etc. this is just a feature of disease, injury, and health. there is nothing unusual or new about it conceptually, it is only the relentless foregrounding of this notion in covid that is new along with the claims that it is extremely common/serious.
but is it?
a challenge in assessing “long covid” is that psychosomatic illness is a real and prevalent issue as is generalized ill health. many feel themselves to be sick and to have general or non-specific symptoms of “brain fog” or “unwellness” or “low energy.”
this has been a longstanding feature of the public and such sufferers tend to gravitate to and ascribe their experienced illness to whatever is popular at present from chronic fatigue to fibromyalgia etc. thus, it would in no way be unexpected for such people to claim “long covid” as it is the non-specific malady currently in the press all the time and for which there is no clinical test to prove or exclude.
the question becomes, how can we separate these two competing (and non-mutually excusive) hypotheses?
this longitudinal study took an interesting and sound-seeming approach to that.
let’s look.
this study was of decent size, 189 people with lab confirmed covid19 12% of whom were hospitalized for it, so this is a pretty salted sample from a severity standpoint. 120 antibody negative controls were used.
“symptoms consistent with PASC” were reported in 55% of the covid-19 cohort and 13% of control.
what makes this study interesting is that they performed not only the symptomatic issues and full medical history but also a physical exam and a set of bloodwork along with neurocognitive assessment.
it looked quite robust.
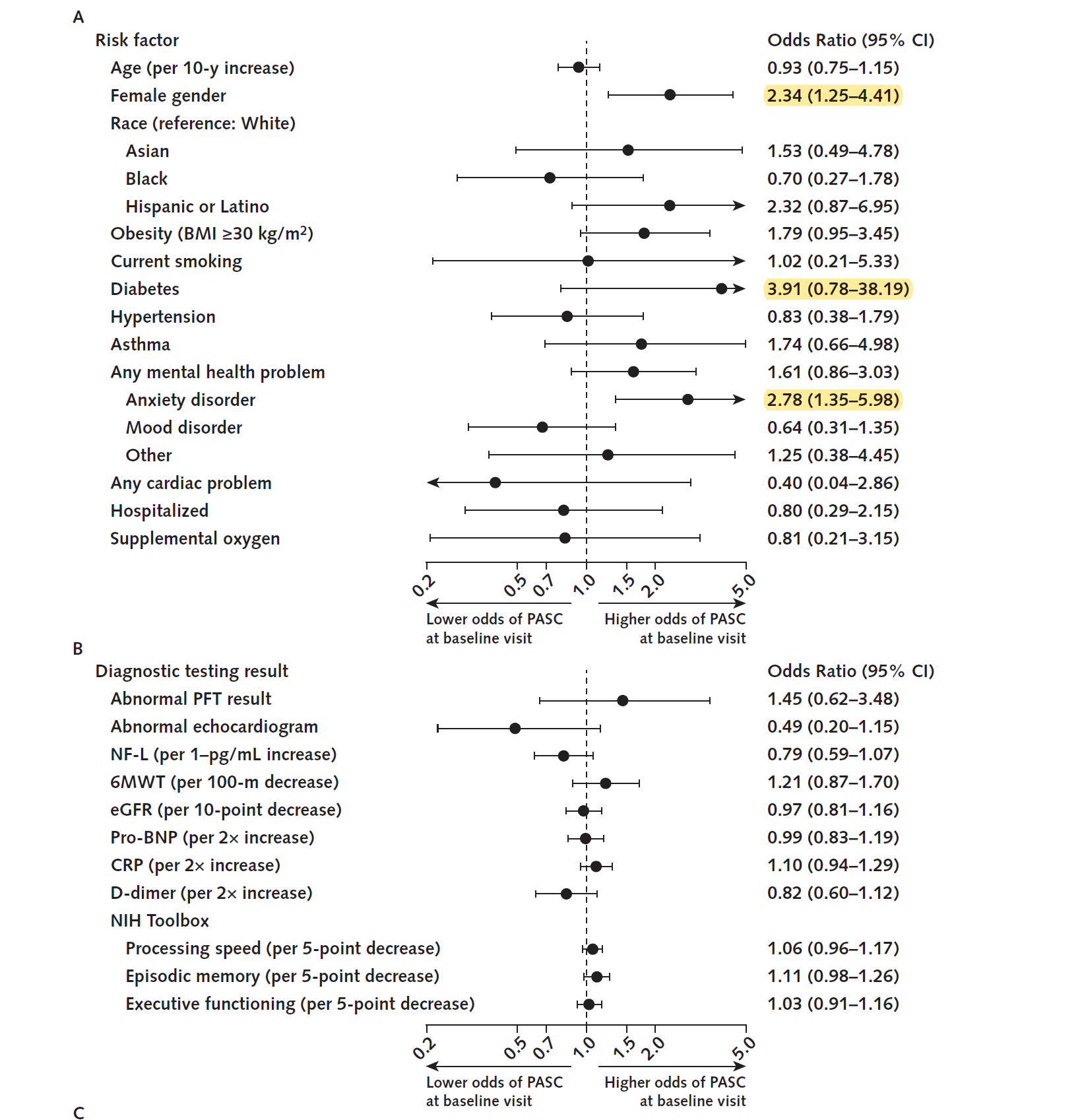
and it led to some really interesting initial data around enrollment, notably, that mental health issues and especially anxiety disorder were extremely common in this group and strongly expressed in PASC.
48% of the PASC group had diagnosed mental health issues. 37.5% had anxiety disorder. this is the sort of alignment one sees in high psychosomatic or attributive conditions.
PASC also expressed at a rate of about 2:1 in women. (only 35.6% of PASC were male)
this also aligns with data from other high psychosomatic or attributive conditions. fibromyalgia (a “trashcan” diagnosis of exclusion that lacks clinical foundation, any known cause/organic disease source or any validating test) looks a lot like this. it’s about 8:1 female (if tested for using tender point analysis and not just highly generalized questions) and has 80-90% overlap with depression.
so, right away, we start to see some of the warning signs of likely mental health involvement in perception of syndrome.
this is very much in alignment with other studies in this space.

actually having had covid was a near useless predictor of “long covid” symptoms but “belief that you had had covid” was a strong predictor of PASC, even in those who were antibody negative. those who had never had covid but thought they did were more likely to claim to have long covid than people who had actually had covid and this held for every symptom except for loss of smell/taste.
but where this new study really got interesting was looking at actual markers of impairment or immune-activation/response/pathology.
the covid group claimed FAR more symptoms. (not surprising as 104 of them were selected for having PASC symptoms)
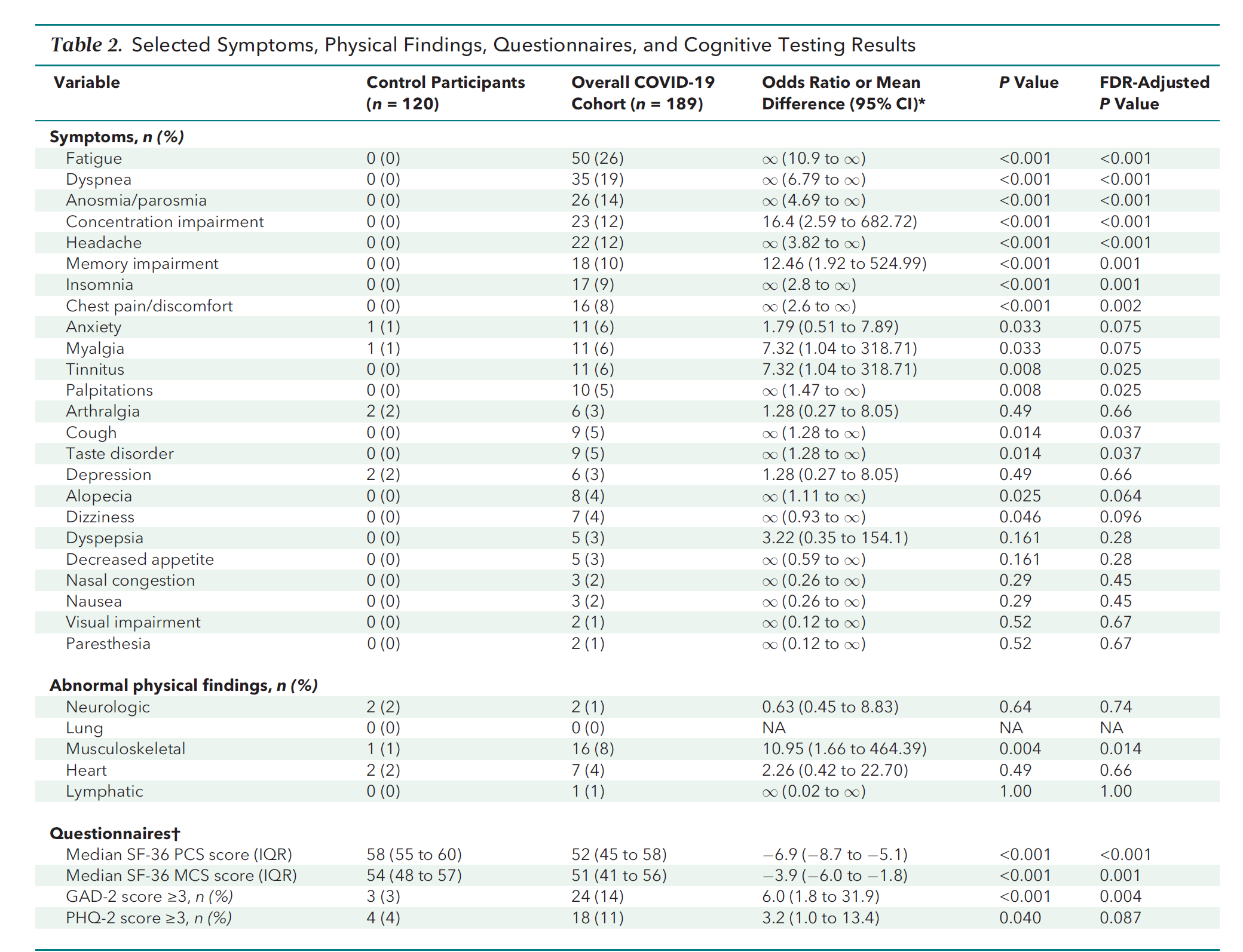
but in terms of actual physical abnormality, there was little variance apart from possibly musculoskeletal which does not seem unexpected given the 38% obesity rate (vs 26% control) in that group.
they reported lower overall health in questionnaires. so, certainly, this group seems to feel less well.
what’s striking is the near total absence of any variation in any of the hard indicators of disease.
if anything, control looked a bit sicker.
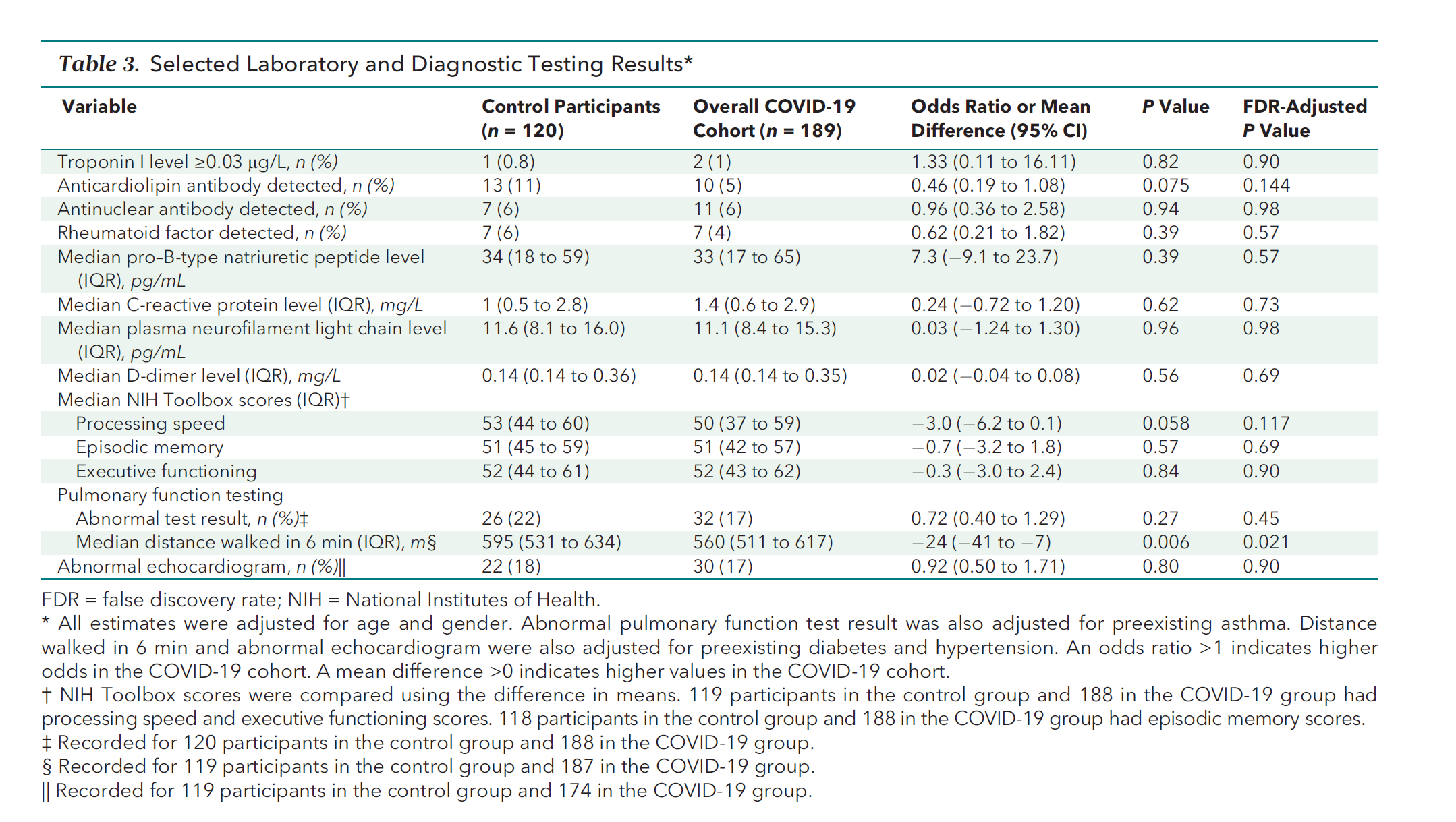
control had higher rates of anticardiolipin antibody (associated with lupus, syphilis, and some other diseases).
control did have better walking speed, but this again may relate to relative obesity rates and did not look material or compelling.
the only other real variance was mental processing speed and, as we lack a baseline, we have no idea if this is caused by illness or a reason people perceive themselves as ill.
immune parameters also showed no variance between those who had had covid and reported PASC vs those that did not (though both varied from control).
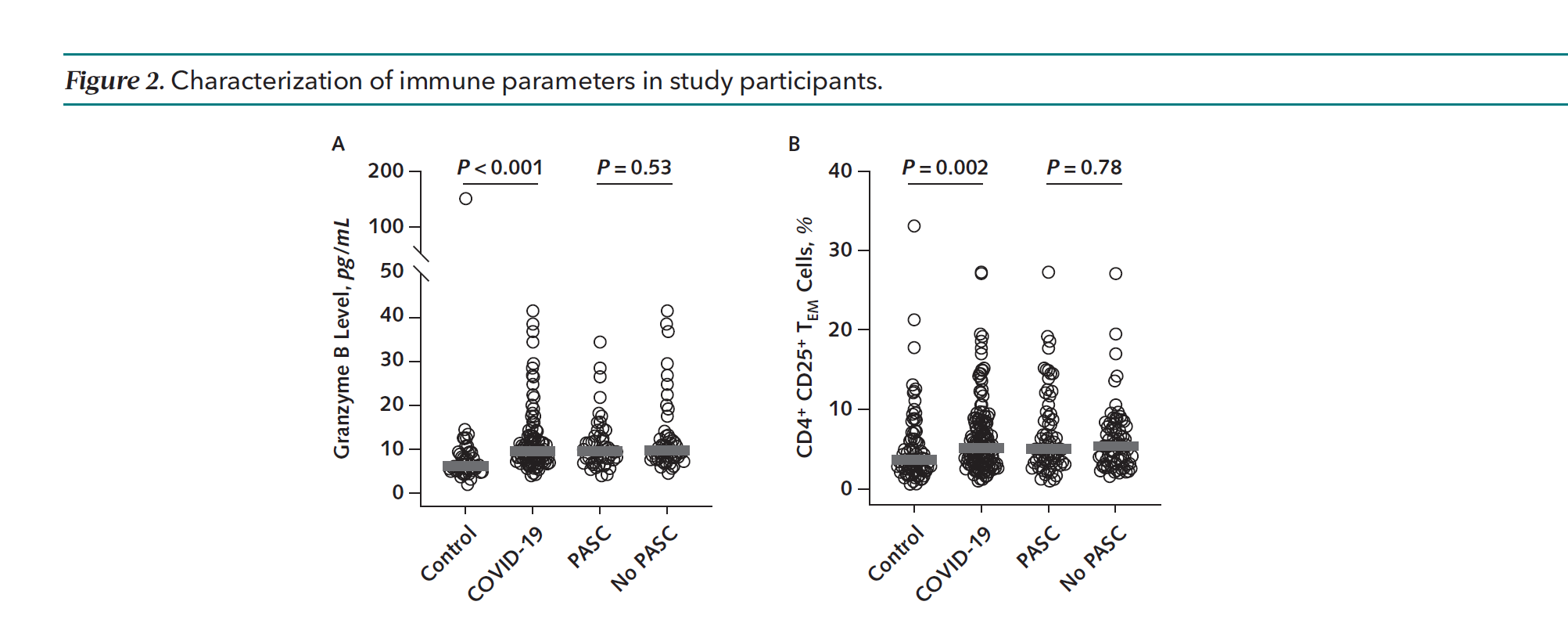
there is really a stunning lack of hard clinical indication that PASC/long covid is an ongoing immune issue.
when tested objectively, this dog is very stubbornly refusing to bark.

the only real risk factors that showed strong association with PASC were gender, diabetes (a disease that has lots and lots of systemic ill effects and that got badly out of control in 2020-2 based on weight gain, drinking, lost exercise, and poor eating) and anxiety disorder.
nothing else was terribly predictive apart from possibly race and i suspect cross confounds there with diabetes etc that make it a difficult signal to read.
taken as a whole, this strongly favors “long covid” being mostly a non-syndrome but rather a sort of catch all for generalized malaise and ill health.
this is not to say that no one has lasting effects from covid, some surely do because this is true of any and all diseases, but it is to say that the prevalence does not appear in any way high or varied from other aliments like flu or pneumonia in any data i have seen and that all the key factors and predictors seem to align with mental over physical cause.
and this matters because the health agencies are making outlandish and unfounded claims about it, generating needless fear, and likely flat out conjuring the syndrome into existence by providing a porchlight against which the anxious and infirm are drawn to batter themselves.
that is not public health, it’s public harm.

worse, it amplifies and elevates the signal of the charlatan class that always emerges to validate and “treat” these chronic “conditions.”
folks like self proclaimed “warrior princess” diana who founded the “covid survivor corps” are preying upon those sucked into this vortex and doing their best to entrap others.
she proudly posts rapid test after test seeking positives/to be sure the other negatives are really negative. but will keep testing! because covid is everywhere!
this sort of poor-calibration and sensationalist scare mongering has no place in public health. it does real harm and invokes inapt reaction, attribution, and risk assessment.
it also prevents the identification of real maladies, especially vaccine injury. one of a cynical mindset might go so far as to wonder if this is why the CDC is so interested in pushing this flimsily fabricated narrative…
after the outright fraud the CDC has pushed as mask studies, it would certainly be of a piece with past behavior.
and it’s long past time they were held to account for it.
Long COVID is part of a chronic condition called Karentitis.
"Long Covid" is largely a coverup for vaccine damage. In an amazing coincidence, many of the symptoms are the same.