


are covid boosters accentuating covid deaths in israel?
assessing the 2 week "worry window" of negative vaccine efficacy

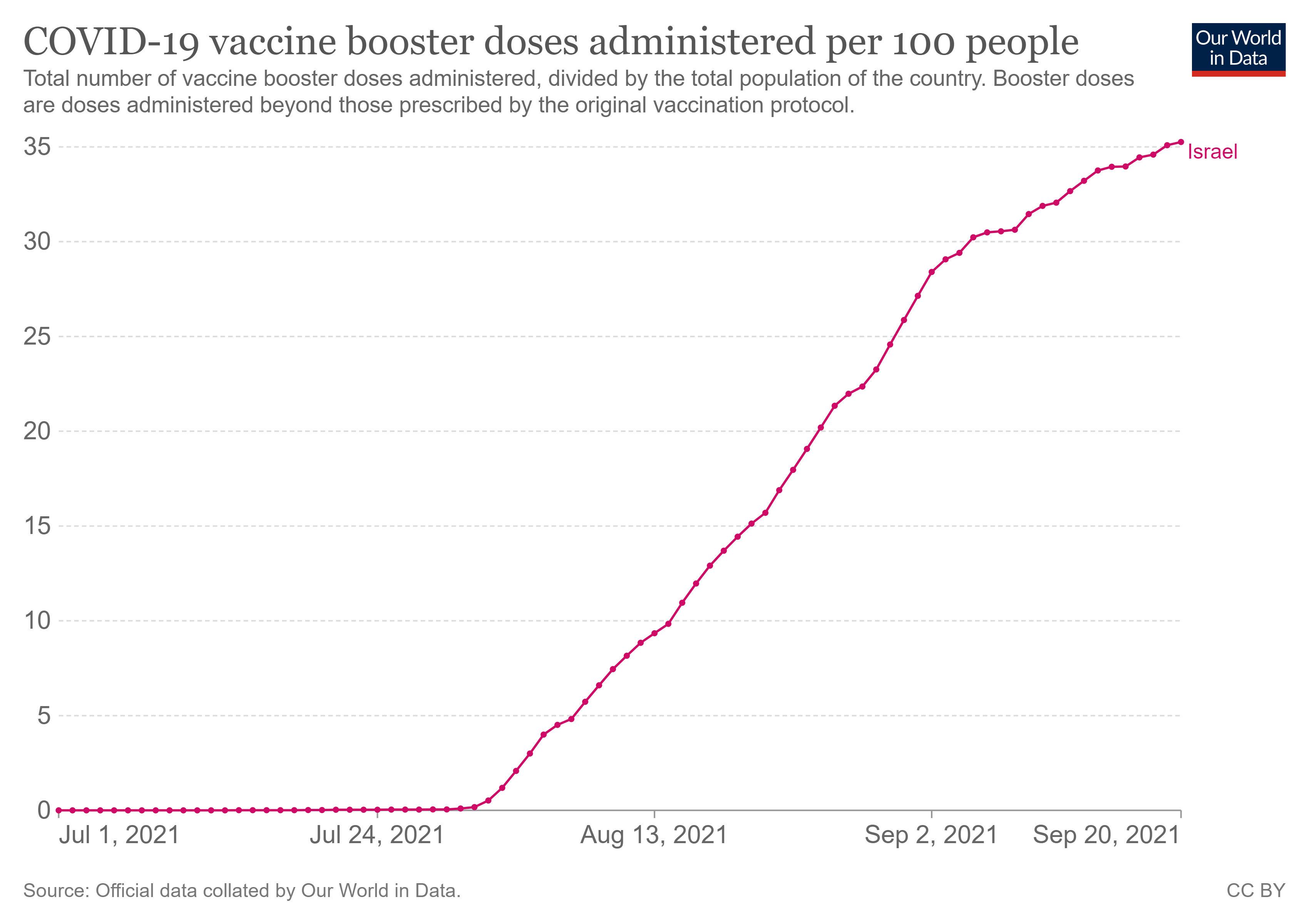
israel remains the canary in the booster coal mine. they are WAY ahead of anyone else on boosters and are one of the only places to mandate them. 35% of the country has had a covid booster shot in a program that started in earnest on august 1.
i spoke about a week ago about the israeli booster data. and then added some further data and some data on palestine HERE. the data was going a bit muddy as we entered yom kippur and reporting was disrupted. it now seems to be starting to clear but i would caution that we really need to watch this over the next week or so as it may not have caught up and it’s possible we’re seeing lags in reporting still.
but provisionally, what it’s showing is very interesting, so let’s look.
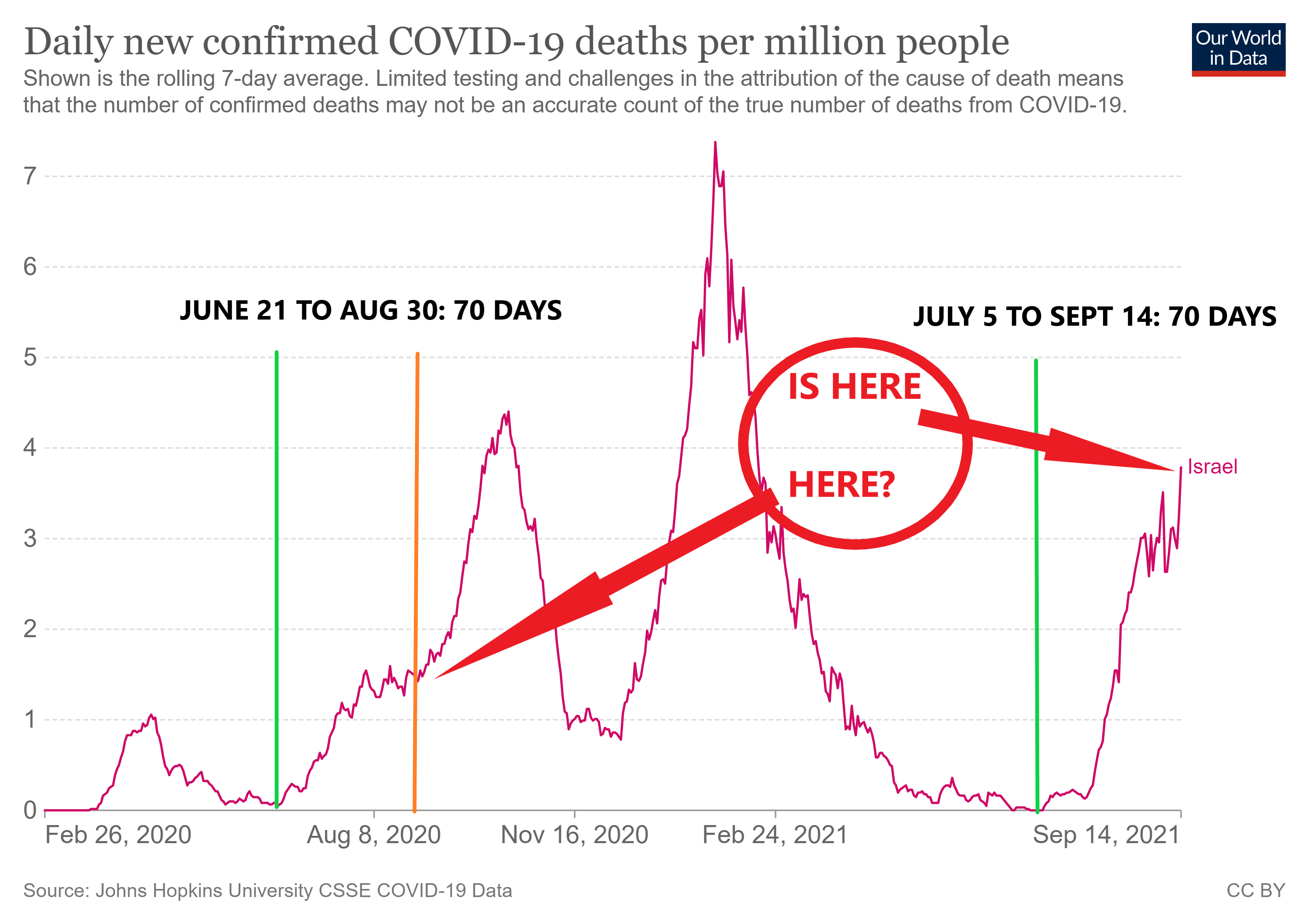
let’s start with this.

first off, i take some issue with the way this data looks to be presented by the IMH. it looks to me like they are truncating the severe case and deaths data for boosters and only counting as “boosted” those 7 or more days post booster. this can cause a severe misallocation of outcomes because boosters, like first doses, appear to have a strong immunosuppressive effect in the first 7-14 days.
and this leads to material data pollution and the inaccurate attribution of bad outcomes that are a direct result of vaccine induced risk enhancement to the “unvaccinated” pool. (it also wrongly boosts apparent vaccine efficacy)
but even so, this data looks quite worrying for the idea that boosters are helping. the “severe case CFR” (SCFR) exploded and moved to a figure roughly twice that of unvaccinated and of the 2 dose vaccinated. this has a provocative consonance with the 100% risk increase seen in the DANISH STUDY during the 2 weeks post administration of dose 1.
the fact that this effect starts to attenuate rapidly after about 10 days also fits very neatly with that risk window.
this data pattern is exactly what you would expect if you were seeing a 14 day window of negative vaccine effectiveness post administration and that D3 was acting just like D1. this seems plausible as D2 comes so closely on the heels of D1 that the body is still loaded with high antibody levels and can manage it. with D3, we seem to be reverting to acting like a first dose.
some have argued that the above chart is reflective of the highest risk people getting boosters first, but this seems like less persuasive explanation to me given how well this ratio fits prediction from what i have termed the “worry window” on vaccines of ~14 days post admin of D1 or D3.
and we see validation here: (graphic borrowed from rafael zioni)

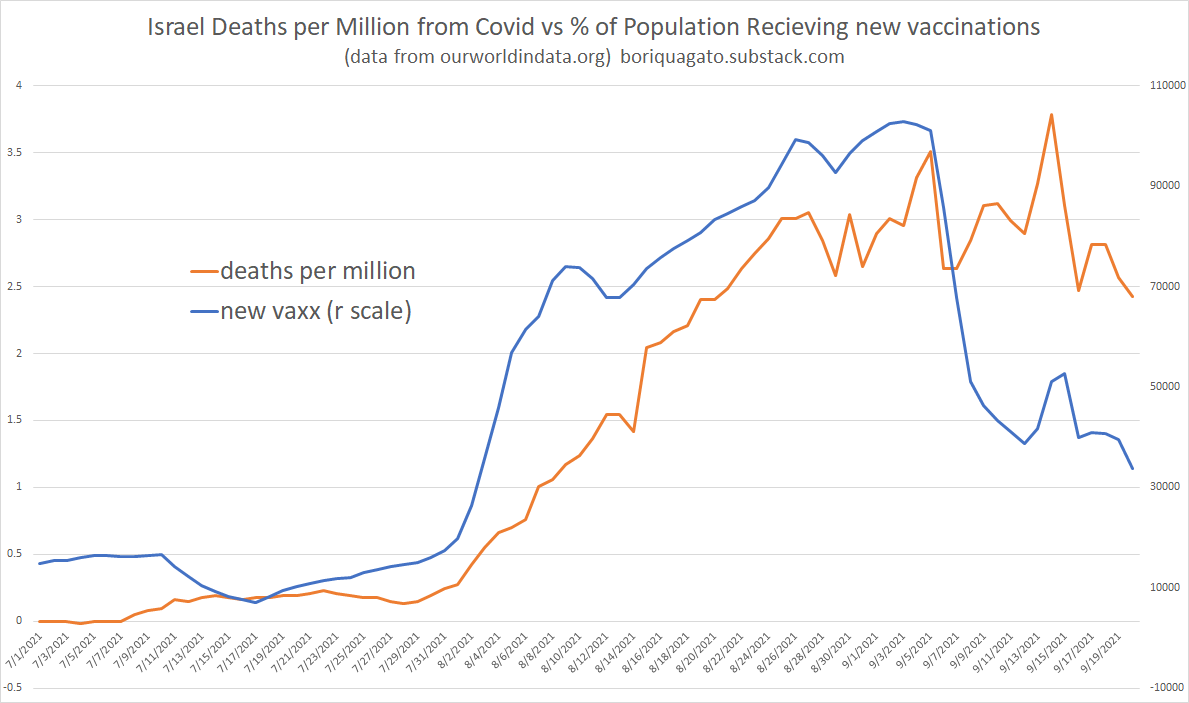
and this sets up what i believe is a useful test of this hypothesis: if i am correct and boosters are causing a 2 week surge in cases and deaths post their administration, then the number of people in the 2 week “worry window” should correlate to death rates. the more people in this risk window, the more deaths should rise and as they fall out, deaths should drop.
we have an unusually good experiment here as it seems that a lot of israelis hurried to get boosters ahead of the holidays (likely to travel and see family etc) and that since then, the rate of new boosters has dropped sharply. (it’s also possible this is a data artifact from holiday reporting so we need to watch out for that over the next week or so)
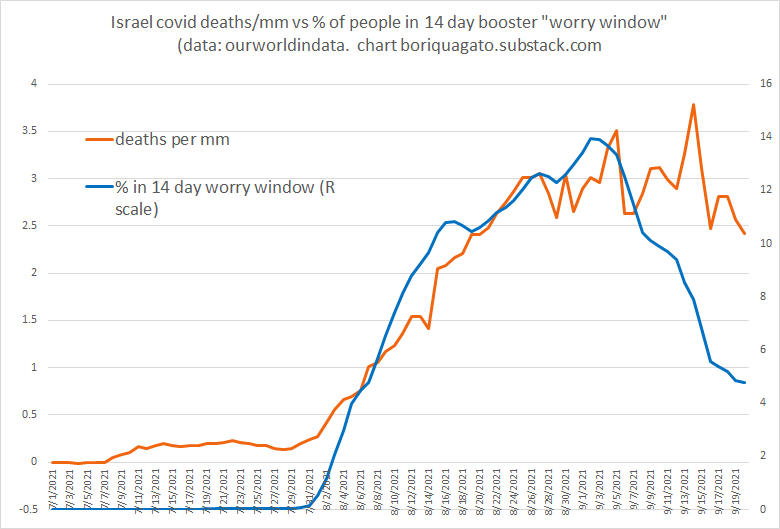
this data is strongly consistent with a 2 week worry window (WW) leading to more deaths.
(and note that this is not data mining as this 2 week window is biologically validated and predicted, so we’re not fishing for correlations, we’re testing a prospective hypothesis.)
we see the size of the WW cohort start to drop sharply after 9/3.
apart from one spike that may or may not be a data artifact from a reporting bolus, deaths seem to track with them and are now breaking down from peak.
if boosters have been the big driver here, then deaths should keep dropping in the coming days (assuming boosters do not start picking up again)
a possible confound to this is the seasonal pattern from last year which surged right about now.
(it’s also possible that we see boosters pick up again and the WW start to expand one more, muddying our experiment.)
so this is the forward prediction we need to track to add confidence to this hypothesis. if size of WW cohort stays low/keeps dropping, deaths should drop as well.
so, now we wait and see.
worth noting is that this is not the first time we’ve seen this in israel.
it happened with dose 1 as well.
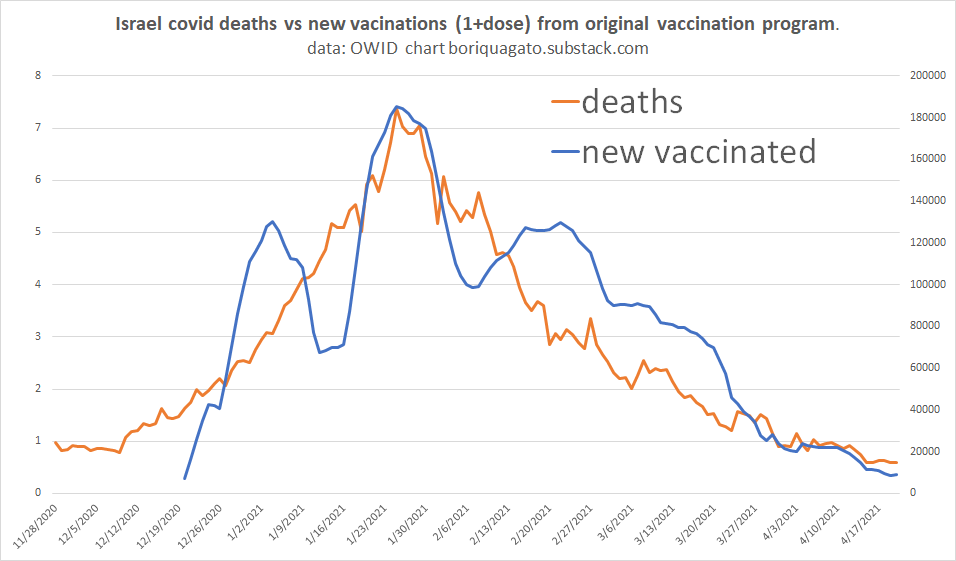
and we can see it track now with “new doses” vs new deaths with doses appearing to lead temporally.
some have questioned whether the effects could possibly be this immediate (so little lag). i believe they can. immunosuppression, especially in vulnerable cohorts or the triggering of some sort of autoimmune/inflammatory reaction can kill very, very quickly. in fact, it’s sort of famous for it.
we can see an interesting anecdotal illustration HERE in a story that really buried the lede.
ostensibly, this is the tale of a school counselor who “did everything right.” she masked, she distanced, she got vaccinated.
they look to pin her sudden hospitalization and death on “going back to work” because this was the “one thing that changed.” but, deep in the story, we see that it was not the only thing that changed. there was another variable in the mix: just days before she got ill, she got a covid booster.
this “confirmation that she had covid before getting the vaccine” feels like nonsense.
who would, if they knew they currently had covid, get the vaccine? what doctor would prescribe that?
this feels assumptive and whitewashy as a doctor not aware of the worry window looks to explain an outcome they fail to understand. was there a test?
but if she did have covid before she got D3, then the immuno-suppression would have been brutal. the disease would have run rampant and unimpeded especially if the neutropenia or suppression of TLR’s 3,7,8 that many have posited occurred. she would have been left defenseless and dying in a few days would not be unexpected.
this is a rough theory and it’s one i am 100% sure nobody wanted to hear.
we were all rooting for vaccines to work here as they have so many other places. but this is a new vaccine type and we’re seeing all sorts of new issues. never in human history has a vaccine been given to so many with so little testing. so, the testing is happening now in societies all over the world. and it’s worth remembering that this was a choice, not a necessity.
it was, in my view, quite reckless and and the fact that we’re having these discussions and seeing such possibilities as these are the direct result of the choice to push a never before used in humans vaccine type with a history of bad side effects into a billion people on the basis of a few months of testing where 6-10 years would have been more normal.
and clearly, those pushing these mRNA vaccines got quite a lot wrong.
it’s clearly non-sterilizing and that alone is cause for serious alarm because leaky vaccines can have dire societal effects. these vaccines do not add to herd immunity and may be worsening spread and even intensifying overall pandemic.
but they also look seriously immuno-suppressive for ~14 days post admin of D1 and it looks more and more like D3 works the same way.
if this is so, boosters are a VERY dangerous game to play, especially in times of high disease prevalence.
and if this is so, we need to know.
this is public health, not a wubbie to pull over our heads.
will keep tracking this and see where it leads…

Recklessness seems to be the new faith-based public health best practice these days as far as I can see. They had a chance to take it slow and reasonable back in December by only allowing the EUA to cover the elderly and comorbid and telling everyone else that they would be fine, this virus is of no additional risk to them relative to normal flu and cold viruses, and even spectacularly great for kids. This was all scientifically established beyond any reasonable doubt in December. Buuuuut … no …. not the global public health establishment (aka the government arm of Big PHARMA). So it was vaxx, vaxx, vaxxity vaxx we go. Gin up the hysteria of “variants”, get those ER and ICU shots from stock footage back on the nightly news. Threaten to destroy people's careers if the don't comply, tell people all their children are going to DIE if they are not vaxxed soon. Complete and total recklessness. And so, here we are, the boosters are coming to the elderly and “compromised” (aka everyone over 16 who wants one) to be delivered just in time for the fall seasonal surges in the midwest followed by the Northeast … perfect timing for the WW.
Naturally, people will blame the lack of masking up in outdoor settings and while walking to the bathroom in restaurants and the “unvaccinated, unboosted” for all of the disease and death that results. Pfizer will announce its 4th boost, now recommended every 3 months. And we will be here again in December. Sigh … this is our new Afghanistan, GWOT.
I understand that neutropenia following D1 is confirmed and not disputed by the vaccine manufacturers, and I agree that immunosuppression can lead very quickly to terrible outcomes.
But I also wonder if this rise in C19 cases and deaths following D1 and now D3 are, in fact, vaccine deaths. We know that the LNPs can travel all over the body and that they were designed to survive the immune assault for a time. It is possible that the PCR tests...even antigen tests...are detecting the vaccine nucleotides...not viral nucleotides.
Yes, severe immunosuppression following D1 and D3 could explain the time compression between diagnosis (+PCR result) and death...so could vaccine injury.
The Israeli health ministry could easily answer the question of immunosuppression with blood tests following D3. Trying to determine where the PCR or antigen tests are detecting vaccine not virus nucleotides is more difficult. And, of course, no one is motivated to look for something they don't want to find.
Thank you for you data analysis and insight. We are all in your debt.