


are leaky vaccines driving delta variant evolution and making it more deadly?
assessing the england data on variants and vaccines. the pieces are coming together.

one of the great fears in any vaccination campaign is that the vaccine can wind up becoming the driver viral evolution and making the virus more dangerous. this is a special concern around imperfect (so called “leaky”) vaccines that are non-sterilizing. such vaccines do not stop spread or contagion of the virus. this means the virus will have lots of chances to replicate.
when you combine this with a vaccine that reduces severity of cases and prevents deaths in the vaccinated, it’s a bit of a perfect storm. you get full spread but break the evolutionary gradient towards mildness that viruses tend to follow (and that protects humanity from them).
all a virus wants is to replicate. “make a copy of me and pass it on.” that’s the biological imperative of the selfish gene. excel at it, you win. fail, you disappear. simple as that.
killing or harming the host is maladaptive to viral spread. it’s like burning down your own house with your car in the garage. now you have nowhere to live and no way to get around. that’s not a recipe for reproductive fitness.

this is a property of the world, not of the viruses themselves. so it applies to all of them, evolved and lab hotwired alike.
so viruses evolve to become less, not more virulent. they do not want to kill you. ideally, they’d like to help you. figure out how to be a useful symbiote, and you get a huge boost in propagation. (mitochondria were probably bacteria that were so useful, all our cells incorporated them.) so seeing case fatality rate (CFR) rise in a variant of a virus is like watching water flow uphill. it’s not supposed to do that and when it does, you need to suspect some external force acting on it.
and we’re seeing water flow uphill here.
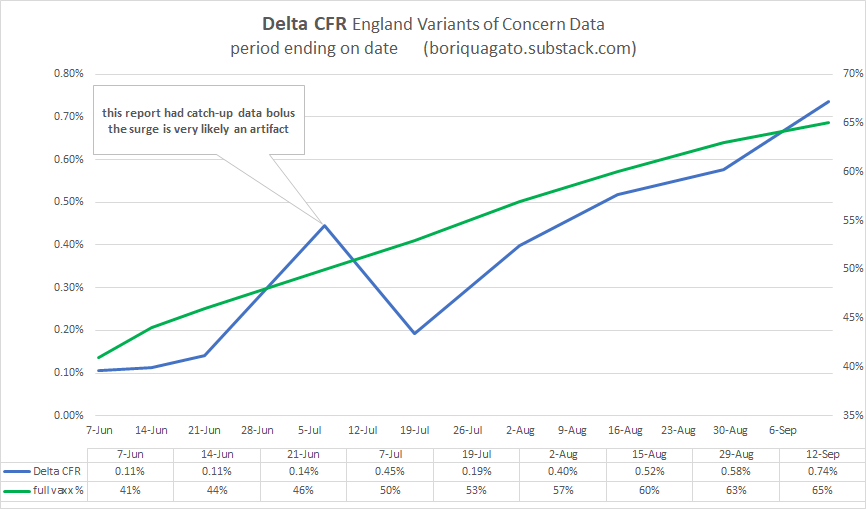
i started with the england variants of concern (VoC) data. it’s the best quality and the best broken out. (the US data is just plain broken. it’s being deliberately scrubbed to prevent analysis like this.) because this data is always aggregated from feb to current period, it does not provide good temporal snapshots, but this can be fixed by subtracting the penultimate report from the current one etc. you subtract report 22’s totals from report 23 and you get just what happened in the last 2 weeks (it used to be a weekly report, now it’s bi-weekly)
what we see is not what one would expect from a virus. none of the other variants (pre vaccine) worked like this. none saw CFR rise like this. and no jump from major variant to variant saw a statistically significant rise in deadliness.
this IS however what one would expect if a virus were undergoing vaccine mediated evolution (as mareks disease did in chickens) and selecting for hotter strains because vaccinated people can carry and spread them and not die.
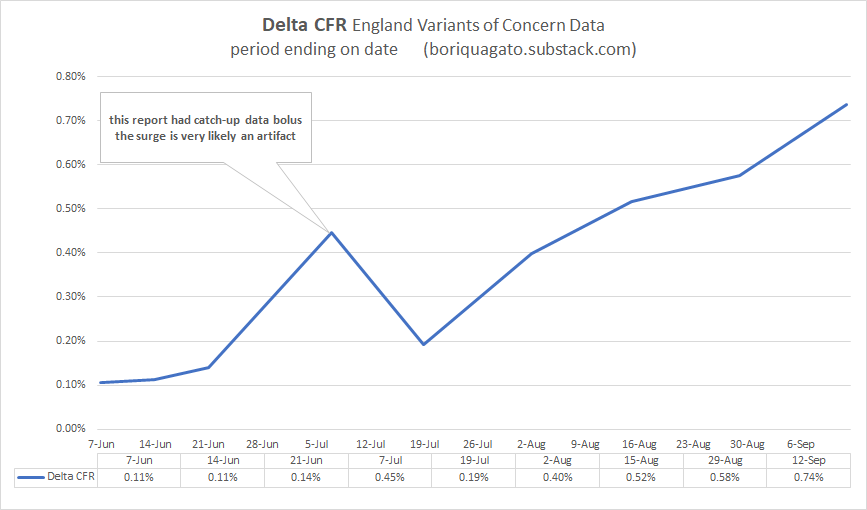
experienced CFR on delta is nearly 7X what it was in the beginning of june and has been galloping since the middle of july.
(note that pretty much all this data has a large artifact in it from the 21 june report (VoC 17). there was a “data-dump” in it where they caught up on a bolus of past data. it’s an artifact, not a signal. best to ignore it. i suspect the curve from mid june to mid july was smooth.)
put simply: this is not good.
delta is rapidly approaching alpha (1.1%) in terms of CFR whereas it used to be 90% lower. (it also means that the reports on delta CFR in these VoC updates are FAR too low because they are a blend of all cases and deaths back to feb, so they are averaging in the low CFR past and are slow to respond to current dynamics)
this is consistent with, but not proof of vaccines mediated evolution. to get there, we need to do better.
so now we need to start ruling things out and validating this claim to see if it’s meaningful.
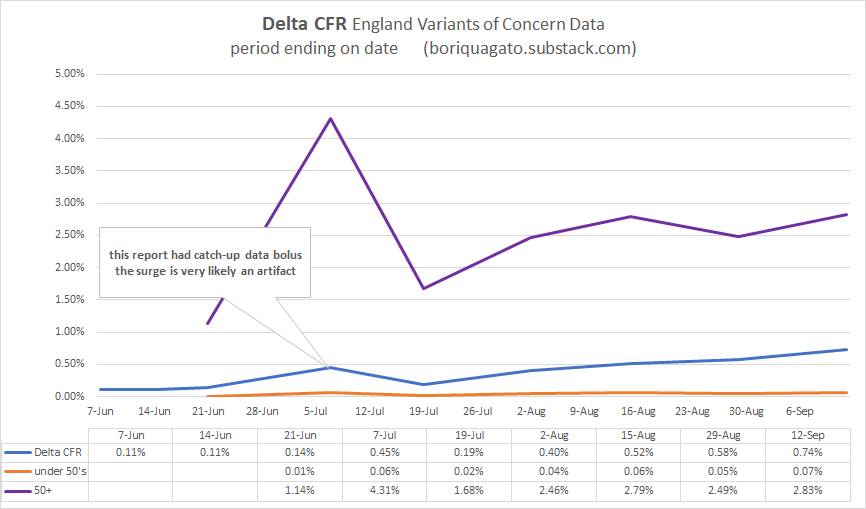
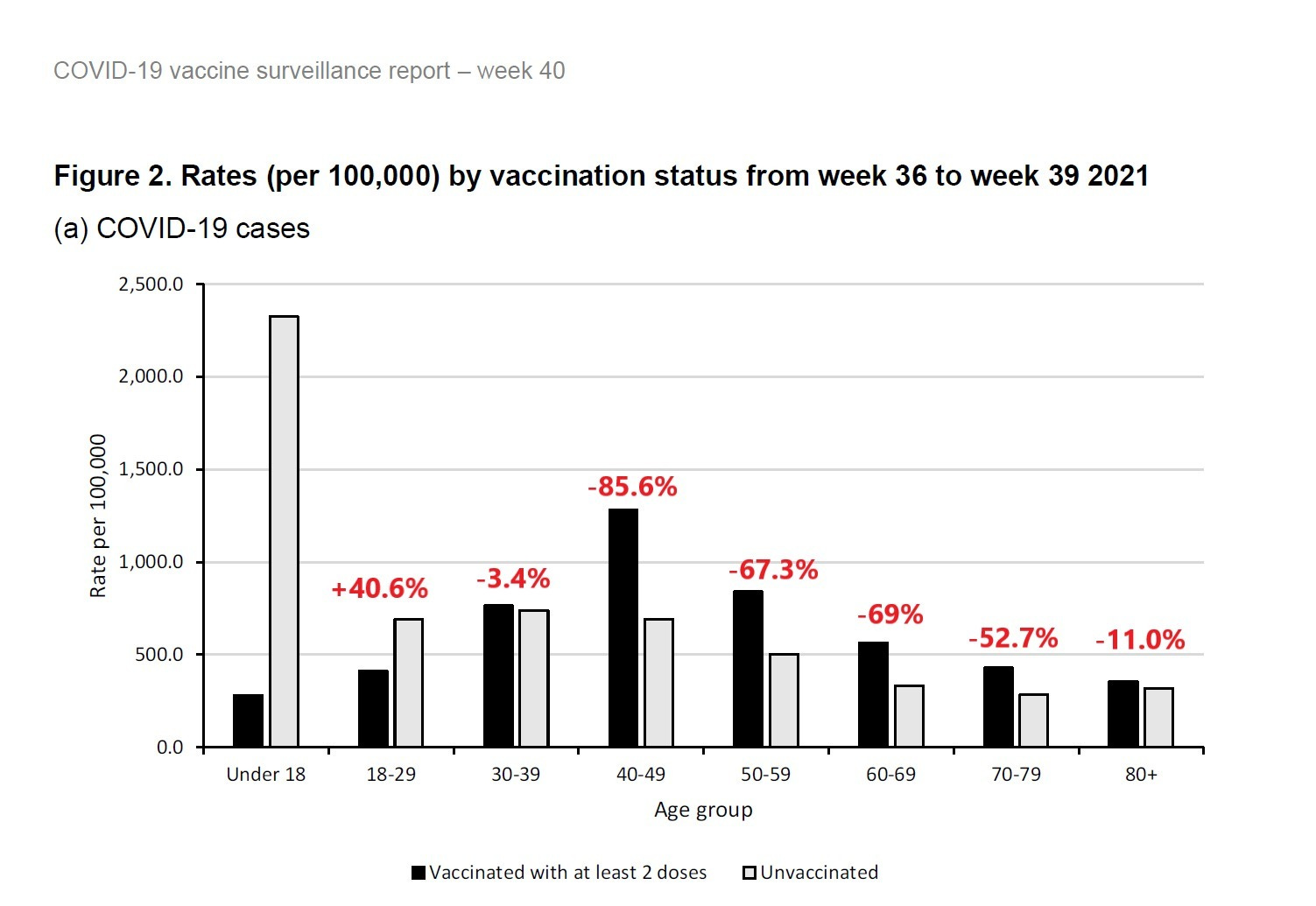
first, it’s not a simpson’s paradox in age data. CFR is rising in over and under 50’s. it’s not mix shift alone. CFR in over 50’s is up 2.5X. it’s up 4-7X in under 50’s.
we’re at about a 3X rise in CFR overall in delta since the summer once we adjust for shifts in age. not as worrying as 7, but still worrying.
and the deaths are real. it’s not made up counting. this can be clearly seen when we comp CFR to the euro-momo Z scores (thoughtfully provided by frequent gato collaborator ben m at USmortality.com. z score is just a measure of deviation from expected all cause deaths. (explained HERE)
alignment is quite strong.
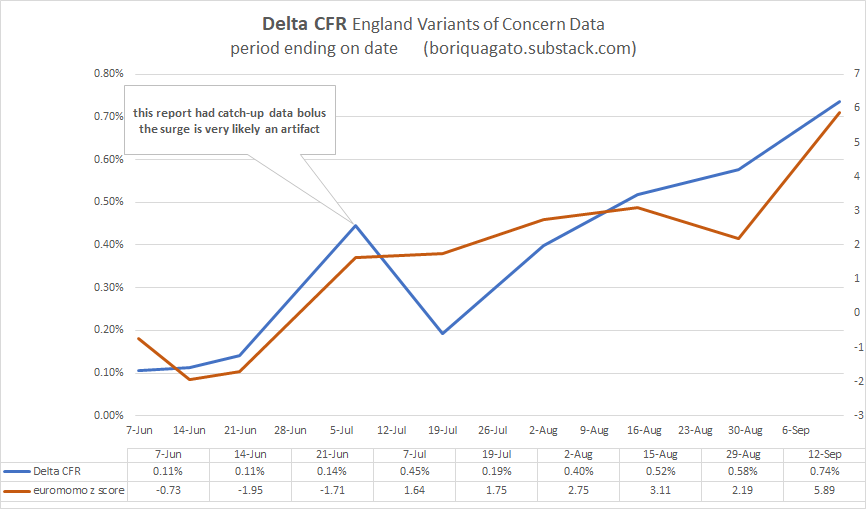
z score was trending negative and spiked to high levels just as CFR really started to ramp up.
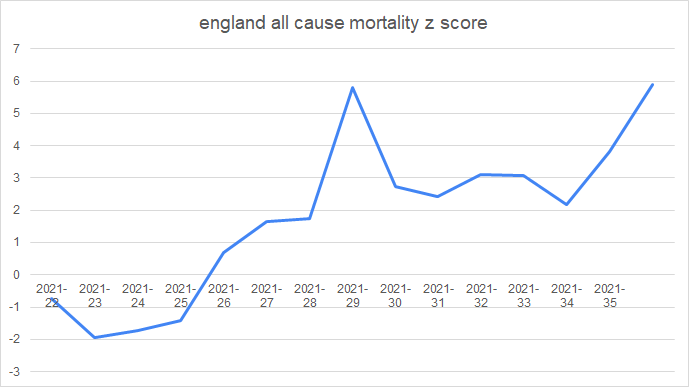
z score for the year can be seen here. starting in wk 22 (may 31) (numbers after the year are weeks)
and given that we know that vaccines DO work to stop deaths in the UK (seemingly in the 50-60% range) it’s even more unexpected that CFR would be rising like this. but it is and the rise in the vaxx rate is not hampering it.
(the precise alignment here is more chart crime than signal, so i’d caution against inferring too much from it)
none of this is what one would expect. not remotely. it bucks evolution, it bucks the other variants, and it flies in the face of late stage pandemic dynamics like increase in acquired immunity (which IS sterilizing), depletion of high risk cohorts, improvements in treatment, etc. all these should be pushing CFR down.
instead, water is flowing uphill.
the question is “why?”
the other day, i discussed ADE (antibody dependent enhancement) where antibodies wind up acting as passkeys for a virus to enter cells and also the fetchingly biblically named OAS (original antigenic sin) whereby preferential training to one antibody response leads to its use against new variants of a pathogen and thereby prevents adaptation to more effective modalities.
note that these two phenomena are by no means mutually exclusive and are actually strongly synergistic.
but are they driving this issue?
i do not not think so.
if they were, we’d be seeing the CFR rise in the vaccinated but not in the unvaccinated and if it were ALL antibodies, we’d be seeing the previously infected getting hit too. but they are not.
we’d also likely be seeing low or negative vaccine efficacy (VE) for deaths. but we aren’t. it’s clear the vaccinated are doing better.
CFR is (and has been) much better in the vaccinated than the unvaxxed in UK over 50’s (the highest risk category). trends are similar, but absolute values durably disparate.
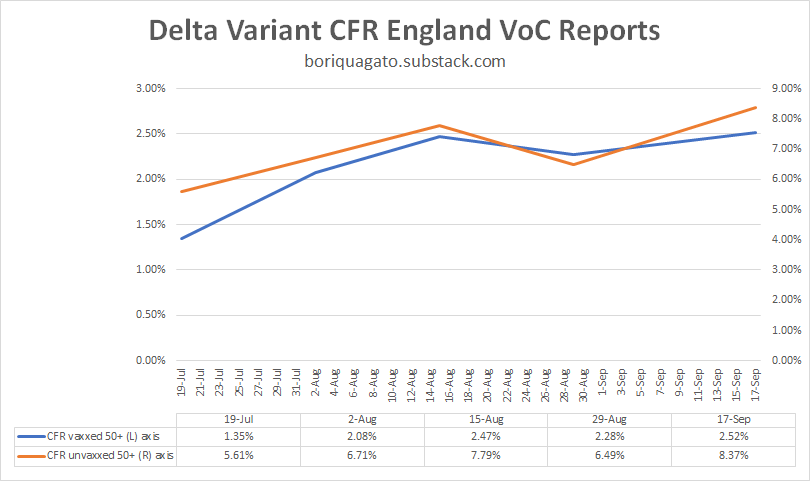
whether and to what extent this is real vaccine efficacy vs cohort bias in a place where 90% of this demographic is vaccinated remains an open issue. it may simply be that only those with the weakest/most compromised immunes systems have not gotten the jab. but this is not really material here.
what IS material is the fact that CFR in the unvaxxed is trending up significantly and so is CFR in the vaxxed. but we’re not seeing many cases of re-infection and almost none of those are serious. this does not look like ADE or OAS as a major driver. if it were, there’s no reason the CFR in the unvaccinated would be rising too.
what this IS consistent with is a variant heating up and getting more and more deadly because it is not checked by normal biological limitations. vaccine mediated evolution (VME) would be very bad news for us.

we can see similar in the under 50’s, though the data here is a bit of a mess as during this period, so many very low risk under 50’s (those under 18) got vaccinated that it moved a material risk profile reduction from unvaxxed to vaxxed. i suspect that is why “CFR vaxxed” dropped. it was not vaccines working, it was the vaccinated category being “salted” with large number of the lowest risk folks around. (it also means that group left the unvaxxed, so you get an effect on both)
so i view this data as much lower quality than over 50’s, but it still looks like VME, not ADE or OAS.
this is EXACTLY what leaky vaccines did in chickens.
(read these links. THIS in particular. it’s important.)
such vaccines change the evolutionary gradient for a virus. instead of becoming less virulent/deadly, they can tend the other way because the maladaptiveness of killing the host is mitigated in the vaccinated population. this is what happened with marek’s disease in chickens.
not only is it now more lethal to them than ebola is to humans, making it one of if not THE hottest persistent disease known (killing 100% of unvaxxed birds in 10 days), but, it’s now a disease so hot that an unvaccinated chicken cannot spread it. they die too quickly. only the vaccinated birds spread the nasty strains of mareks. they’re the only ones who live long enough to shed virus.
““Previously, a hot strain was so nasty, it wiped itself out. Now, you keep its host alive with a vaccine, then it can transmit and spread in the world,” Read said. “So it’s got an evolutionary future, which it didn’t have before.”
this is an awful lot of puzzle pieces snapping together and i think we’re really starting to see what this is a picture of.
leaky vaccines that stop severe illness and death but not spread look to be affecting the evolution of the covid 19 virus.
this is an established, predictable, and well supported risk from such vaccines.
this has become my leading hypothesis.
it also explains why we’re seeing such a large rise in deaths relative to cases and deaths and hospitalization overall in so many places. it’s the virus adapting to a stressor we put on it and becoming much more dangerous as a result.
the CFR is a function of the virus, but the virus has become a function of the leaky vaccines.
and it also means the vaccine is protecting no one. yes, it seems to have 50-60% protection against death. but what good is that against a CFR that’s up 300% or more (and rising)? everyone is worse off.
negative VE’s on spread are accelerating cases and this is multiplicative with higher CFR. this is the nightmare scenario and no one is left better off as a result. the CFR among the high risk vaccinated groups is way up too.
everyone is harmed but the brunt is borne by the unvaccinated which perversely winds up looking like better vaccine efficacy. the very fact that vaccines made everyone worse off but spread the misery unevenly makes it look like vaccines are a good idea.
it’s just simple math. if we do something to one group that makes their death rate rise from 1 to 2 per 100 but that also makes the death rate in another group rise from 1 to 4 per 100, that looks like a VE of 50%. in reality, it’s killing 100% more vaxxed people and 300% more of the unvaxxed.
mistaking that gas pedal for the brake and pushing ever harder when you fail to slow would represent an accelerating disaster curve.
that’s the problem with relative measures that ignore absolute changes. you can hide all manner of calamity in such analyses.
it’s still, or course, possible that i’m wrong, but this is looking more and more like it has to be the answer. i can find nothing else fits the facts and the facts themselves are weird enough that “it’s just normal” does not look like a satisfying explanation either and we have enough features here that we can really start testing our puzzle pieces. this one aligns in an AWFUL lot of places.
for something this odd to happen, it takes a truly uncommon exogenous stressor.
i’m just not seeing what else it could be than vaccine mediated selection for hotter variants driving pernicious delta evolution.
so, i’m putting this out to you all to see if you can find some other explanation for what’s going on that fits these facts.
looking forward to the peer review as, honestly, i hope i’m wrong here. this is not an outcome that anyone wants. it’s the nightmare scenario both as a pandemic and as a political horror in the making as if this was an “own-goal”, what would the experts and politicians than pushed this plan not be willing to do to avoid accepting the blame?
because this is career or pharma franchise polonium, and that’s if you’re lucky.
let’s keep at this. one way or the other, we need to know.
the facts do not care about our feelings and epidemiology data is a lousy fabric from which to spin a wubbie to hide under.
we need to get at the truth.
(even if it makes us make a face like this)

Coffee in hand and I’m realizing I’m not crazy for wanting to catch Delta before the SHTF and hospitals are overrun and panicking. Maybe we go back to the trend chicken pox/ COVID parties before it gets worse so we get more folks with natural immunity?
There are a few key drivers you have put aside, that in my opinion change drastically the perspective.
If one talks about Mareks disease, one needs to consider that chickens are by definition naive immunologically to the disease (as recent newborns) and also living in a high dose/high transmission environments. In other words, there's no buffer to contamination in the community, so the doses are crazy high and the chicken are literally petri dishes for anything being produced into this high density environment. The collective immunity being close to zero, the high viral density in the environment is most lethal element.
With Covid19, we are far from these circumstances. We don't live in feedlots (not yet!), and we had high pre-existing collective immunity. We weren't naive to SARS-COV2 as proven by tens of studies that showed high levels of cross-reactive T-cells/B-cells etc... Hence the asymptomatics.
Now, if one believe Mareks theory, as the outcome of a non-specific immunization, widely spread cross-immunity would have pushed for more immune evasion... we didn't see this at all for at least 12 months. On the contrary, SARS-COV2 swept thru Hyderabad (up to 70%) in 2020 with 9 out 10 infected not aware of being infected.
I would like to question the validity of 2 strong assumptions you are building upon. You are making the strong assumption that:
a) these intramuscular vaccine work: I personally don't see how that is possible with an intramuscular shot that will not address any of the root causes of severe Covid: obesity-induced ACE-2 density (a viral fertilizer), very delayed immune response (lacking dendritics) tied to immunosenescence (the "alarm" is off), and mucosal cell-to-cell propagation (Abs are useless then). As demonstrated in the "Recovered", only a mucosal vaccine could trigger sterilising and effective immunity by triggering protection in the entry point of the virus.
The "magic trick" of changing the vaccine cohort baseline by depleting it of the frailest individuals - who effectively succumb to AEs - has clearly biased the RCTs (very visible in the Israeli trial) stripping the vaccine cohorts of the most sensitive population and "improving" its performance, while at the same time worsening the unvaccinated cohort and the severity of the virus.
b) CFR is corrrect: You are assuming these people are dying of Covid, not with Covid, of mislabelling or worse of the vaccine. (1) we know how outrageously overcounted the cases/deaths have been in many countries (the US notably). So cases being garbage-in/Garbage-out, one cannot build a serious scientific argument on it. (2) it is quite obvious, that many have died from intravenous injection/leak of the vaccines into the bloodstream. The systematic simultaneity of Covid deaths with vaccination is simply impossible from a probability standpoint: UK, Israel, Chile, Vietnam, Seychelles, Laos, Cambodia...The autopsies, the VAERS data, the discrepancies in the UK data from January onward (in 2021, patients don't call 111 before dying...wtf?!)...
I would add that variants aren't stopping recovered from fighting it off easily...Variants are a fallacy to sell yearly vaccines. The wide epitope repertoire both for T-cells and abs are sufficient to be immune as proven by the iconic article of the La Jolla Institute in January 2021.
We have all been trying to avoid the looking at reality in the eyes...
The idea that variants explain 2 or 3 waves in the same season makes no sense. Depleted susceptibles cannot get replenished in a week or so like we 'have seen in the UK, in Sweden, in Hungary, countels countries....so what are those cases? well one very possible hypothesis, is that they are vaccine-induced Covids tied to direct injection in the blood vessels by untrained nurses and doctors, and/or that the LNPs leak back into the bloodstream. Whichever the reason, having 20-50 billion LNPs starting to transfect endothelial cells in a concentrated fashion in microvessels, followed by T-cells destroying square meters of the vessel walls is not good. I would add that, the very elderly - the very ones we are trying to save - would also have delayed response, and would thus produce enormously more spike proteins than immune valid adults.
Finally, I would like to point a different risk tied to generalized vaccination of an already immune population. As a sophisticated bio-software, the immune system has likely a feedback loop to adjust its response: if one is already immune, following vaccination, the immune system would necessary launch a very wide response (intramuscular infection is way past a mucosal attack), T-cells would rapidly destroy those transfected cells and a large number of Tcells would have to anergize pretty quickly. Done twice, it is highly probable that the vaccine would adjust down its response to avoid off-target damage and waste of ressources. Generalised to a population that could mean the vaccines could have collectively reduced our immunity level, which would mean the ambient viral density would be much higher going forward...When one acknowledges that dose and immunity are the 2 most critical factors in mortality, that could be disastrous.