



updating the UK data on VE vs delta
variants of concern reporting and concerns about variants

i did THIS analysis a ways back to look at UK vaccine efficacy vs delta variant. i chose UK because they have the best (and very nearly the only) data on variants of concern and actually split it out by vaccination status allowing us to aggregate the full effect of vaccination from dose on onward. i believe this to be critical because it appears that there is a 2-3 week period of highly enhanced vulnerability to covid post dose 1. most countries are only reporting efficacy for “fully vaccinated” (dose 2 more than 14 days ago (some use 7)) for reasons laid out in detail HERE i find this extremely misleading (at best) and outright dishonest (far more likely).
the UK variants of concern data can be hard to parse for VE because its timeframe is so long. each bi-weekly report goes back to feb 1 and aggregates all data.
however, this allows us to see individual 2 week slices if we simply subtract one report from another. last time i looked at data from aug 15 to aug 29. this time, i subtracted briefing 22 from briefing 23 to get the data presented below.
this is subset data of just confirmed delta breakthroughs. to get to vaccine efficacy (VE), i normalized all data to what it would be if it were the whole population so that cohorts could be compared.
the simplest way to think about VE is this:
if 100 unvaccinated people all have X happen to them and it happens 70 times in 100 vaccinated people, that’s a 30% VE. it stopped 30% of X.
if the vaccinated group gets 130 instances of X, then VE is -30%. it made it 30% worse.
the data gives us this:
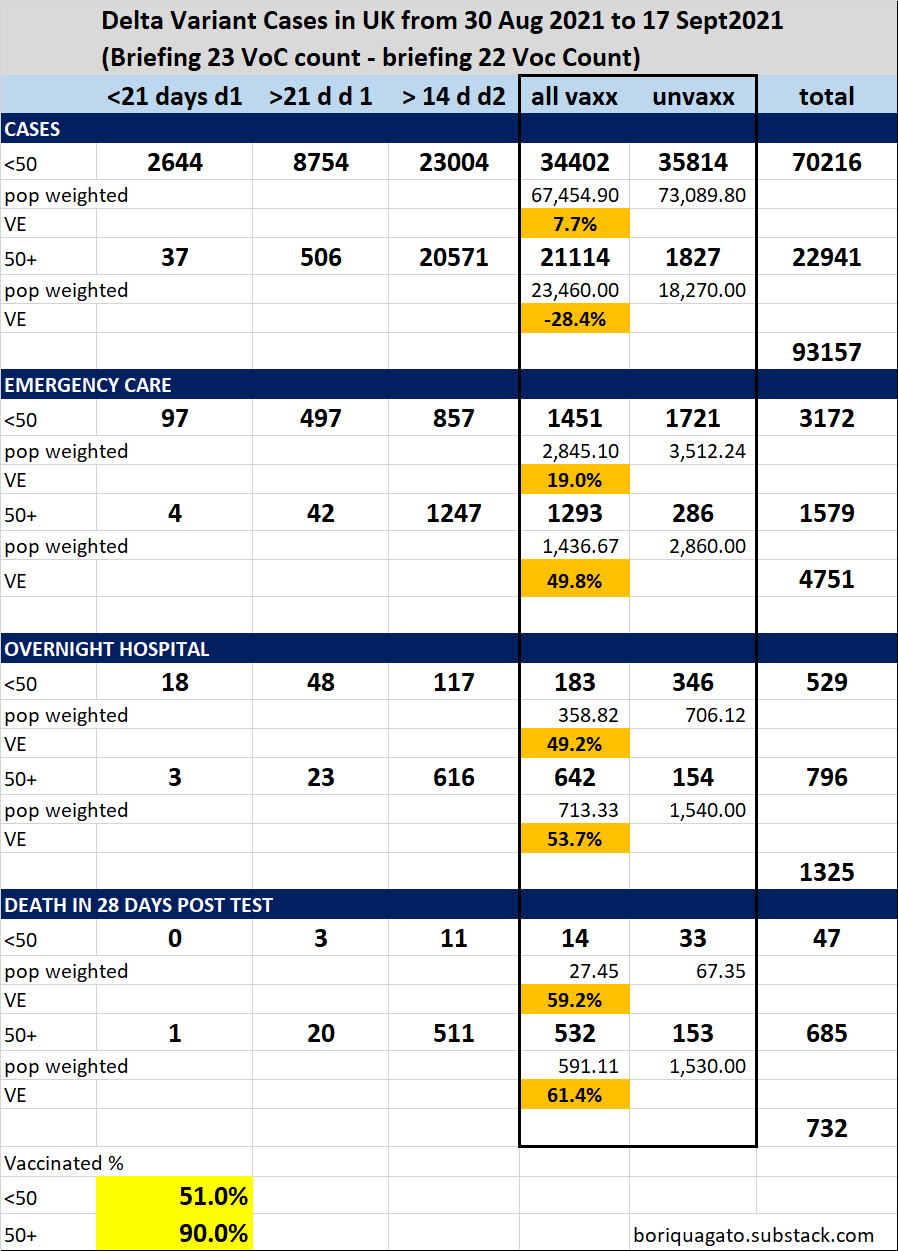
it looks broadly the same as last time. the one meaningful difference seems to be that VE for cases in under 50’s jumped form -15.6% last time to 7.7% this time. meanwhile VE for cases in over 50’s dropped from -16.3% last time to -28.4% now.
i’m not really sure to what to attribute this odd set of changes or why it diverges so much from the vaccines report data explored HERE. it is subset data of just established variant cases, so it may be injecting some sort of bias that i cannot quite figure out. (if folks have thoughts on this, would love to hear them)
vs the last fortnight (aug 15-29), VE for emergency care dropped slightly
23.1% in under 50’s dropped to 19%
52.6% in 50+ dropped to 49.8%
overnight hospitalization VE was mixed
39.6% rose to 49.2% in under 50’s
56.1% dropped to 53.7% in 50+
deaths VE seemed better overall
51.9% rose to 59.2% in under 50’s
59.2% rose to 61.4% in 50+
honestly, i suspect that most of the changes here are within error bars with the exception of:
the rise in cases VE for under 50
the drop in vases VE for over 50
the rise in overnight hospital VE for under 50’s
possibly the rise in protection vs death in the under 50’s
this led me to wonder if something significant changed in under 50’s. it seems perhaps so.
the count of those 16-18 getting vaxxed rose sharply, likely for back to school. this is an incredibly low risk cohort. shifting them from unvaxxed to vaxxed is like taking a 0 you got on a quiz and making it into a 100. it does not need to be a big % of your overall grade to have a big effect on the aggregate mark and because VE is relative between cohorts, the effect is doubled here.
this actually gives me more confidence in this analysis as managing to pick up the back to school vaxx signal makes it look like it tracks well.
so this leaves us very much in the place we thought ourselves before.
we have a leaky vaccine that is ineffective at best and likely counter productive in stopping spread.
that vaccine IS effective in mitigating severe cases and deaths (though not nearly so effective as claimed)
this efficacy looks to be fading over time
many see this and jump to “you need this vaccine to protect yourself and protect hospitals.”
but i see severe issues with this claim. a leaky vaccine that prevents severe cases is, in many ways, the WORST possible outcome.
such vaccines change the evolutionary gradient for a virus. instead of becoming less virulent/deadly, they can tend the other way because the maladaptiveness of killing the host is mitigated in the vaccinated population. this is exactly what happened with marek’s disease in chickens. not only is it now more lethal to them than ebola is to humans, making it one of if not THE hottest persistent disease known (killing 100% of unvaxxed birds in 10 days), but, it’s now a disease so hot that an unvaccinated chicken cannot spread it. they die too quickly. only the vaccinated birds spread the nasty strains of mareks. they’re the only ones who live long enough to shed virus.
”Thus, in accordance with the imperfect-vaccine hypothesis, vaccination enabled the onward transmission of viruses otherwise too lethal to transmit, putting unvaccinated individuals at great risk of severe disease and death”
this raises the pressing question of “is this same intensification of virus happening here?”
unfortunately, signs here point to yes.
i’ve posted this graphic of delta CFR several times.
it should not be trending up without some sort of exogenous forcing.
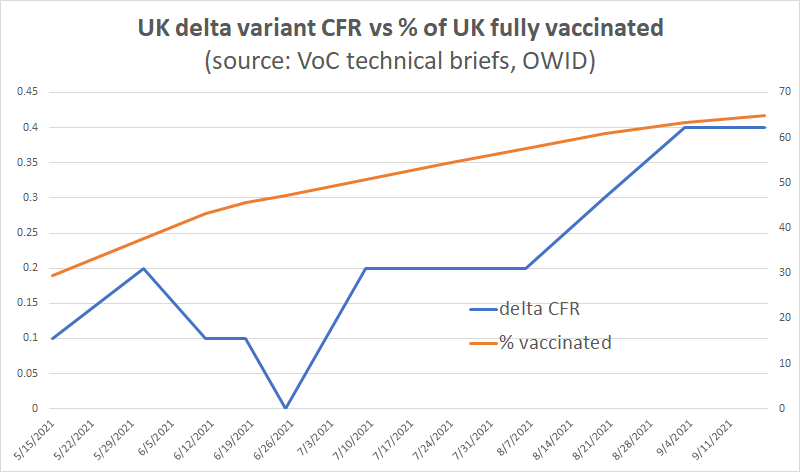
i have also realized that i did this wrong and this chart understates the CFR of delta and the extent to which it has risen. it’s using reported delta CFR from the variants of concern reports. but that CFR is cumulative back to february, so the signal is deeply damped as it gets averaged with long ago data.
i cut it for the periods from aug 15-29 and from aug 30 to sept 17. what i saw worried me.
CFR was 0.62% in late aug. it rose to 0.79% in the first half of sept. this is nearly double the 0.4% aggregate being reported and shows worrying growth at the margin. this is EXACTLY what one would expect if we were seeing imperfect vaccine driven evolution. it also may answer the riddle of why deaths are up ~100% relative to cases in the US north. a variant that got 100% hotter vs where it was would do it.
i’m going to have to break up the UK reports and get bi-weekly slices going back a way to get at this and plot it and it’s going to take some time because they are not set up to provide east data grabs. (sigh) but this one looks important.
if delta CFR is tracking the way i think it is, we have a big piece of the puzzle and a more or less smoking gun on vaccine driven evolution.






I'm listening to Steve Kirsch https://skirsch.io He does statistical analysis as well. He advises that we need to consider all cause mortality--not just reducing Covid deaths. For if we save the life of a Covid patient, but then another person dies from the vaccine, we haven't really saved any lives. This is a common problem when evaluating drugs and procedures in medicine. For example, a highly toxic chemotherapy drug will be applied. It is successful according to the measure of "reducing size of tumor." However, the patient's immune system was damaged by chemotherapy and, as a result, they died of pneumonia. They are still counted as a success. Kirsch reports that vaccines were not successful in reducing mortality in trials. This is the bottom line.
This has been my greatest fear for a while. The virus evolves to become more virulent among the vaccinated, but the vaccine helps the vaccinated survive. Then that more virulent strain hits the unvaccinated, and deaths start climbing. Nobody in a position to do anything about it gives a sh*t, because, hey, their fault they didn't get the shot. Good luck even getting a hospital bed if there's triage. Scary.