


vaccine effectiveness: assessing the duke data
there is no sound evidence of vaccine efficacy here but lots of data being mishandled and controls ignored or absent.

cliff notes:
the duke data is being widely discussed and, to my mind, widely misinterpreted
those vaccinated got covid at the same rates as those unvaccinated. there is no evidence of sterilizing immunity nor prophylaxis and moderate evidence of a lack thereof
the lack of hospitalizations is entirely predictable and the base case assumption even in a disease and vaccine naïve population in this age group over a one week period.
this means that claims of “no hospitalization” do not diverge from even a highly slanted base case assumption and cannot support a claim of vaccine efficacy in mitigating severity.
this does not mean they did not mitigate severity, it means this data cannot prove they did. (absence of evidence is not evidence of absence) this is an important distinction.
there is also, as so often seems to be the case, no discussion of risk reward here. just because a vaccine mitigates severity does not make it a desirable intervention. we must also assess risks, harms, and side effects.
this cost benefit analysis has generally been unfavorable among the young and healthy.
discussion:
many have been discussing the duke data. i’d like to weigh in as i find claims that this data proves vaccines are working to be wanting. it does not support such a claim (though neither does it refute claims of severity mitigation)
let’s take it from the top:
98% of students and 92% of faculty are vaccinated.
“In the first week of classes, 304 undergraduates, 45 graduate students and 15 employees tested positive for COVID-19. All but eight of these individuals were vaccinated, and the vast majority of them are asymptomatic. A small number have minor, cold- and flu-like symptoms, and none have been hospitalized, according to the university.”
so now we can do some math:
304 undergrads test positive out of 6,542. 4.6% in a week.
45 grad students test positive out of 9,009. 0.5%. why this is so much lower is an interesting question to which i’m not sure i have a good answer. possibly relative testing rates and social activity? were undergrads all tested twice or more (especially athletes) and grads mostly missed?
15 employees out of 1,235 tested. 1.2%
2.3% overall of individuals tested resulted in a positive per full test data here.
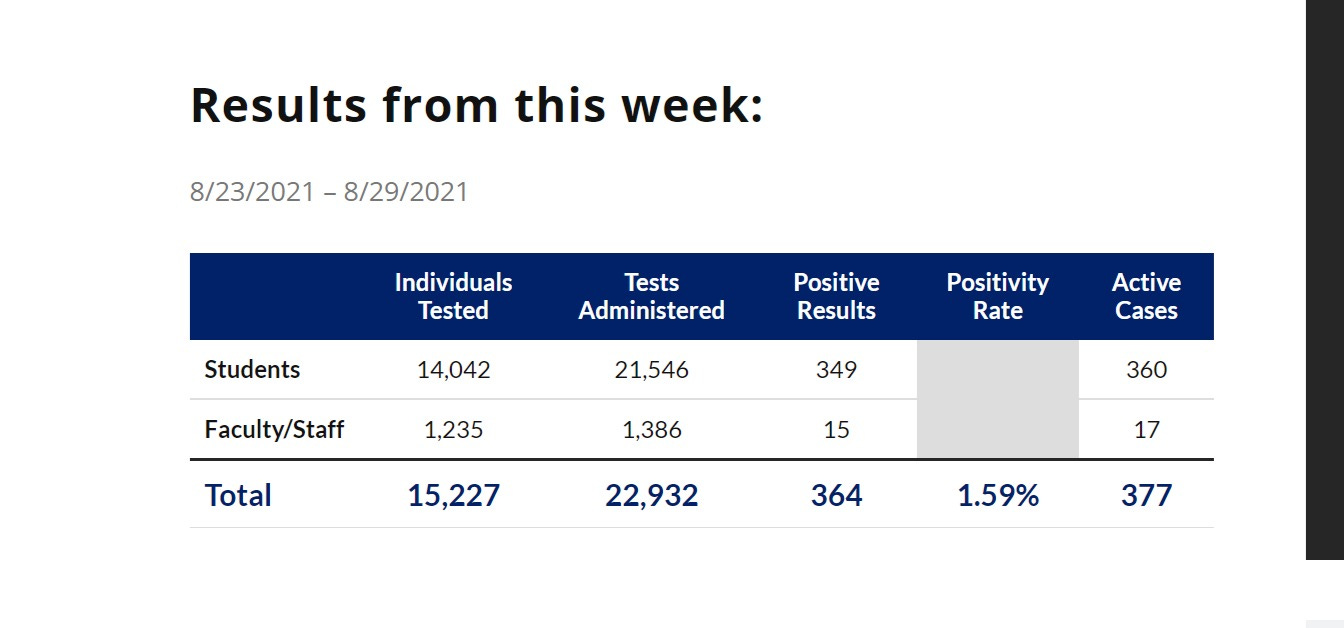
(note that what it calls a positive is per test, not per individual. avg person was tested 1.5 times in this week and that with 15,551 students and 14,042 individuals tested, over 1,500 were not tested at all.)
so did vaccines work? well, it’s hard to say without a control group, but we can try to fashion one based on aggregates.
98% of 14,042 students vaxxed = 13,761.
92% of 1,235 staff vaxxed = 1,136.
total vaxxed = 14,897 out of 15227 = 97.5% vaxxed.
346 cases. 8 were unvaxxed.
so, 2.3% of cases were unvaxxed and 2.5% of population is unvaxxed. that’s functionally identical and shows no curve separation that would be outside of error bars.
this implies no evidence of prophylactic benefit in the vaccinated cohort vs the unvaccinated.
the evidence that these vaccines provide low or no sterilizing immunity after the first couple months seems to continue to mount. but we mostly already knew this.
but what about mitigating severity? how is that working out?
many have claimed that the lack of hospitalization and severe cases shows vaccines are working. i do not think so.
this data does not give us enough evidence to really fashion a control group. it looks like none got very sick, even the unvaxxed. this is to be expected in this age group.
but we can try to synthesize a control group. i will do so by providing every benefit to the duke cohort because it’s easy to make a mess with these retrospective combinations and i’d like to steel-man the case for vaccine efficacy.
i will use as a baseline full societal hospitalization by age group using this cumulative data aggregated by statista.
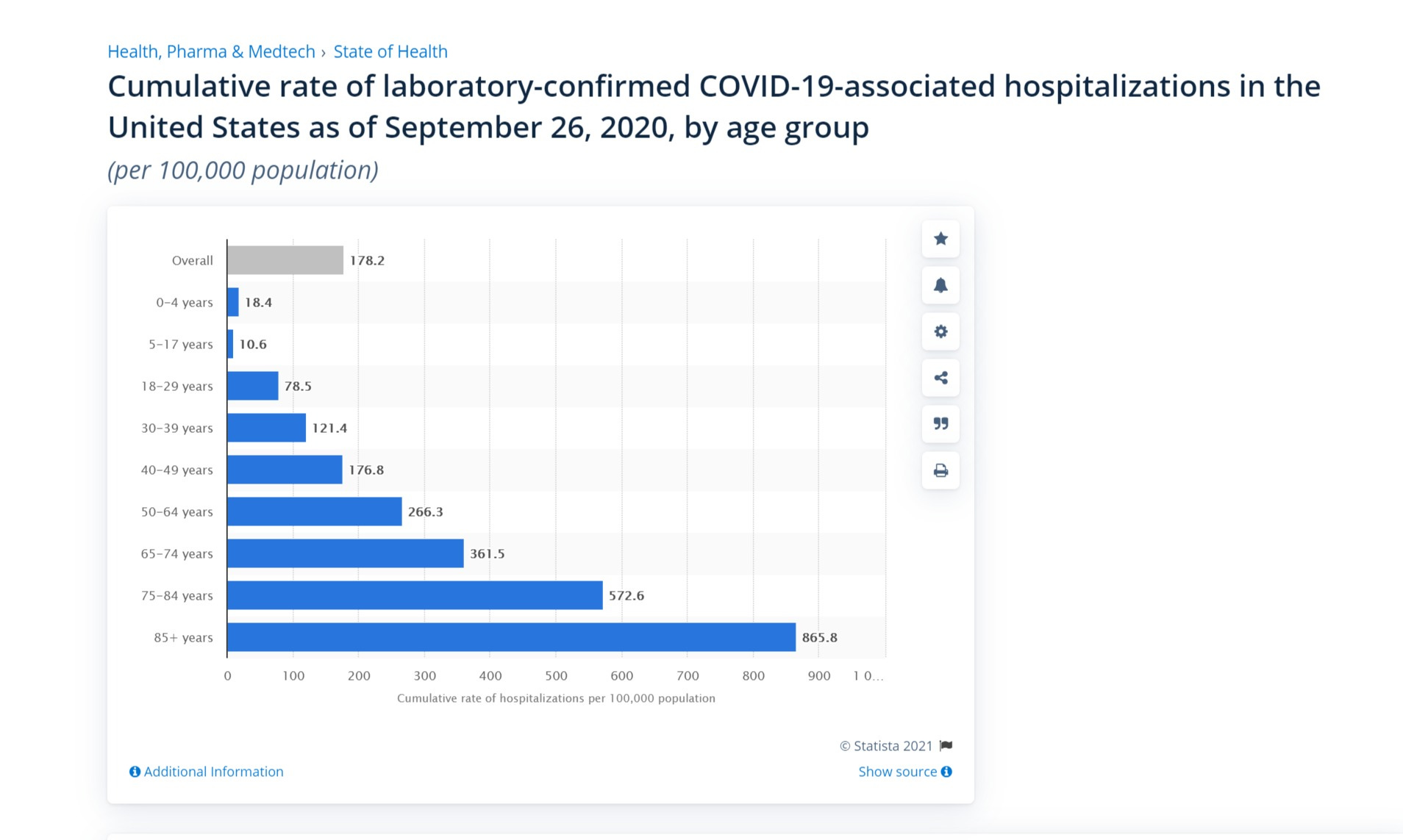
this is data over 27 weeks in 2020 including a winter and summer peak. it’s also in a fully unvaxxed community with far less acquired/recovered immunity than today as it includes the very beginnings of covid. (you’d expect this it be considerably lower today just through acquired herd immunity build and “dry tinder” cohort depletion)
we’ll use the 18-29 years group as it’s closest and because it stretches older than college gives the college cohort further advantage.
78.5 per 100k societal rate is 2.9 per week per 100k.
so, with 6,649 undergrads, you’d have a base expectation of .19 hospitalizations per week or, to put it another way, and 81% chance of having none even in a risk enhanced vaxx and disease naïve population.
yet even with all this stacking in favor of the “vaccines worked” hypothesis, this data simply does not get anywhere near the “proves it worked” threshold.
in today’s population, even sans vaxx, it would be even less likely you’d see one and college students are probably healthier as an average than their age peers as a whole as the very sick do not go to university. it’s almost certain to be over 90% or even 95% chance of no hospitalizations if we risk adjust by health and prior exposure to covid/immunity development over the past 17 months.
grad students got far fewer cases for some reason. i have no solid explanation. perhaps it’s just less contact with others/parties, etc. or lower relative test rates or some combo. it seems plausible that undergrads and athletes were tested a lot and grad students, especially those off campus, far less so. it would appear that at least 1,500 were missed entirely. i’m guessing those were not undergrads.
we can add them all in to the undergrads and get 14,042 students tested overall, but we’d still only expect .4 cases per week from a fully naïve population and thus would expect considerably thus less now.
so there is a 60% chance of “no hospitalizations” even in worst case. in a more realistic case, it’s probably more like 80-90% even without vaccines.
so, again, there is just no real signal there or any proof they worked.
this does not prove they did not work, perhaps they did. absence of evidence is not evidence of absence. but science is about hard evidence and what we can, with confidence, claim from data and this data is simply not sufficient to support either the claims that vaccines stopped spread or that vaccines reduced severity of infections.
it’s also not enough to just point to efficacy even had it been in evidence.
all health decisions are cost/benefit decisions.
vaccines are no different and when they fail to show sterilizing immunity, the argument that you owe it to others falls apart and perhaps the argument that you are posing greater risk to others comes into play either by enhancing transmission of more virulent pathogens or by allowing high levels of viral load to occur on mucus membranes without symptoms creating a new class of vaccinated superspreaders. this is an open and ongoing debate.
but what of the individual? even if your vaccine does not protect me to what extent does it protect you and to what risks does it expose you to confer such protection?
here the data is not favorable to risk reward.
among the young, mRNA vaccines are 20X (or more) likely to put a 12-15 year old in hospital than actual covid.
it’s roughly 3X with the 16-25 year olds that comprise college campus age.
and the pfizer data from their 6 month follow up looks unfavorable for nearly all young healthy people (under about 50).
overall, vaccinating 22k people stopped 29 severe cases of covid and perhaps 2 deaths, though it may likely have caused more deaths from reactions than it stopped from covid.
this was at the expense of maybe 4000 extra related adverse events, at least 110 of them severe. so you have a 110 severe AE cost to 29 severe covid savings. this could easily be 262 to 29 if we rule out the alleged “severe reactions” to saline injections that are claimed. (this seems a suspicious claim)
this seems to make vaccines a very debatable topic for healthy people in terms of efficacy vs risk.
as ever:
this is not medical advice. i’m here to provide information, not to tell you what to do.
ask your doctor, but go armed with data and questions.
healthcare is always and everywhere a cost/benefit decision.
only you can make choices for you and being engaged in and informed about your own health decisions is a life habit that will pay enormous dividends.
it’s one worth cultivating.
"ask your doctor, but go armed with data and questions."
I guarantee that the regular reader of boriquagato is more knowledgeable about Covid, risk factors, mRNA vaccines and the efficacies of NPIs than your average doctor.
I have on my computer a graphic from last year's colleges. It's a big long list of schools, totaling 70,000 "cases" resulting in 3 hospitalizations and 0 deaths.
How would we even know the vaccine was working on these people?