




Discover more from bad cattitude
did BA.4-5 interacting with vaccines cause the death spike in portugal?
circling back to assess the outcomes of our natural experiment

about 3 weeks ago, there was an interesting hypothesis going around that the rapid rise in BA.4-5 in portugal was interacting with high rates of vaccination and boosters to create a sort of vaccine optimized predation as the virus shifted further to use hoskin’s effect/OAS/antigenic fixation to preferentially attack the those most heavily affected by these inoculation regimes. this was posited to explain the sudden rise in deaths.
in some ways, this idea was highly plausible because that’s how virus mutates when selective pressure from leaky vaccines is applied. in others, it was more doubtful as becoming more lethal is evolutionarily maladaptive for a virus. more contagious is strongly selected for, but more deadly tends to result in less spread. killing the host is like burning down your house with your car in the garage.
there was some provocative data with high vaxx portugal and low vaxx south africa both getting BA.4-5 but only portugal getting a deaths spike.
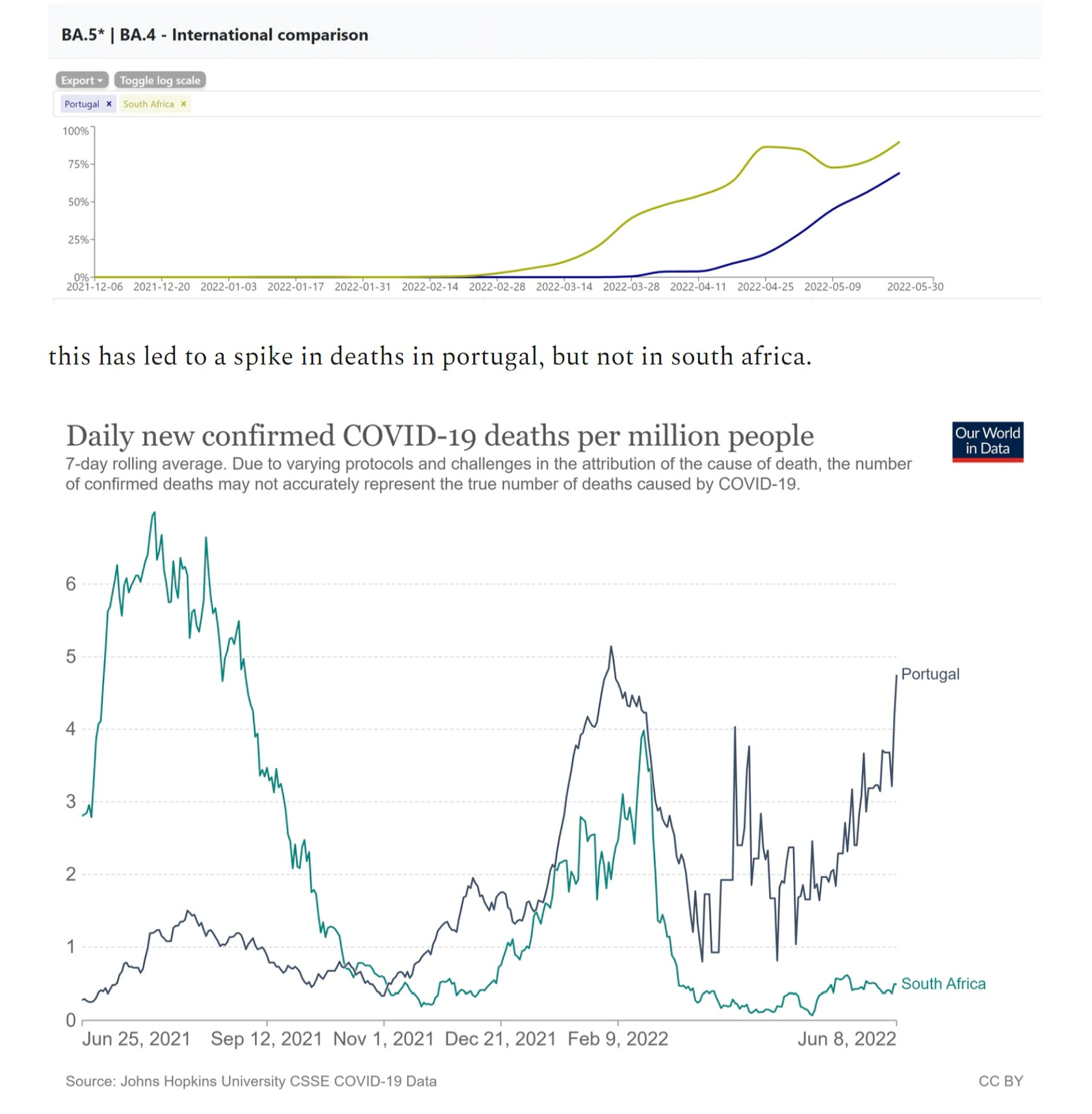
but you have to be VERY careful with data like this. 1,000 things could be driving the difference and presuming that it must be one’s hobbyhorse is a great way to get things wrong.
and this is where the notion of falsifiable/testable hypotheses comes in.
i made some efforts in this direction about 19 days ago:
spain has vaxx rates very similar to portugal. it occupies the same geography. and BA.4-5 were becoming dominant there about a month after portugal.
this looked to provide a good natural experiment:
you can read the whole setup here.

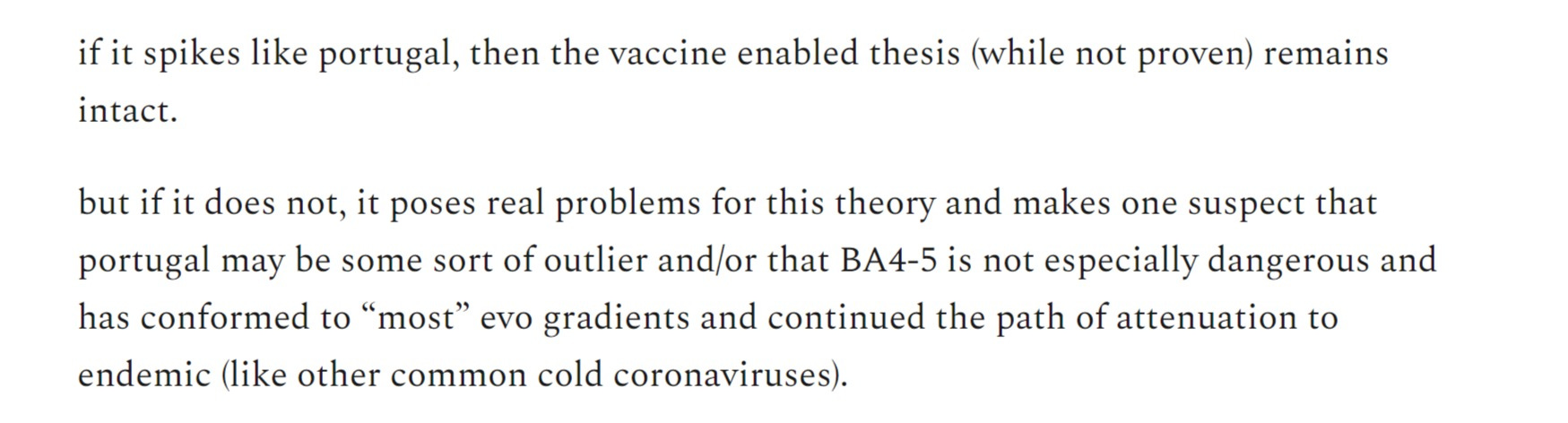
well, it’s been ~3 weeks and the timing looks correct to see how this turned out. i will add the UK as a third check.
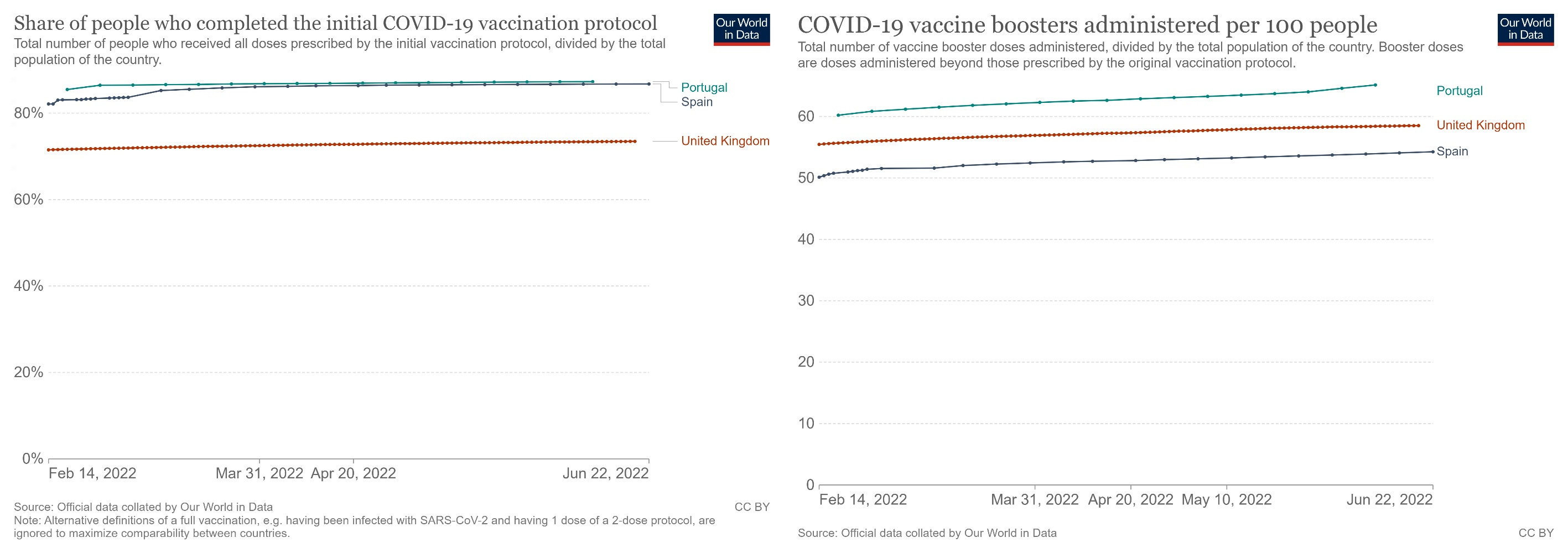
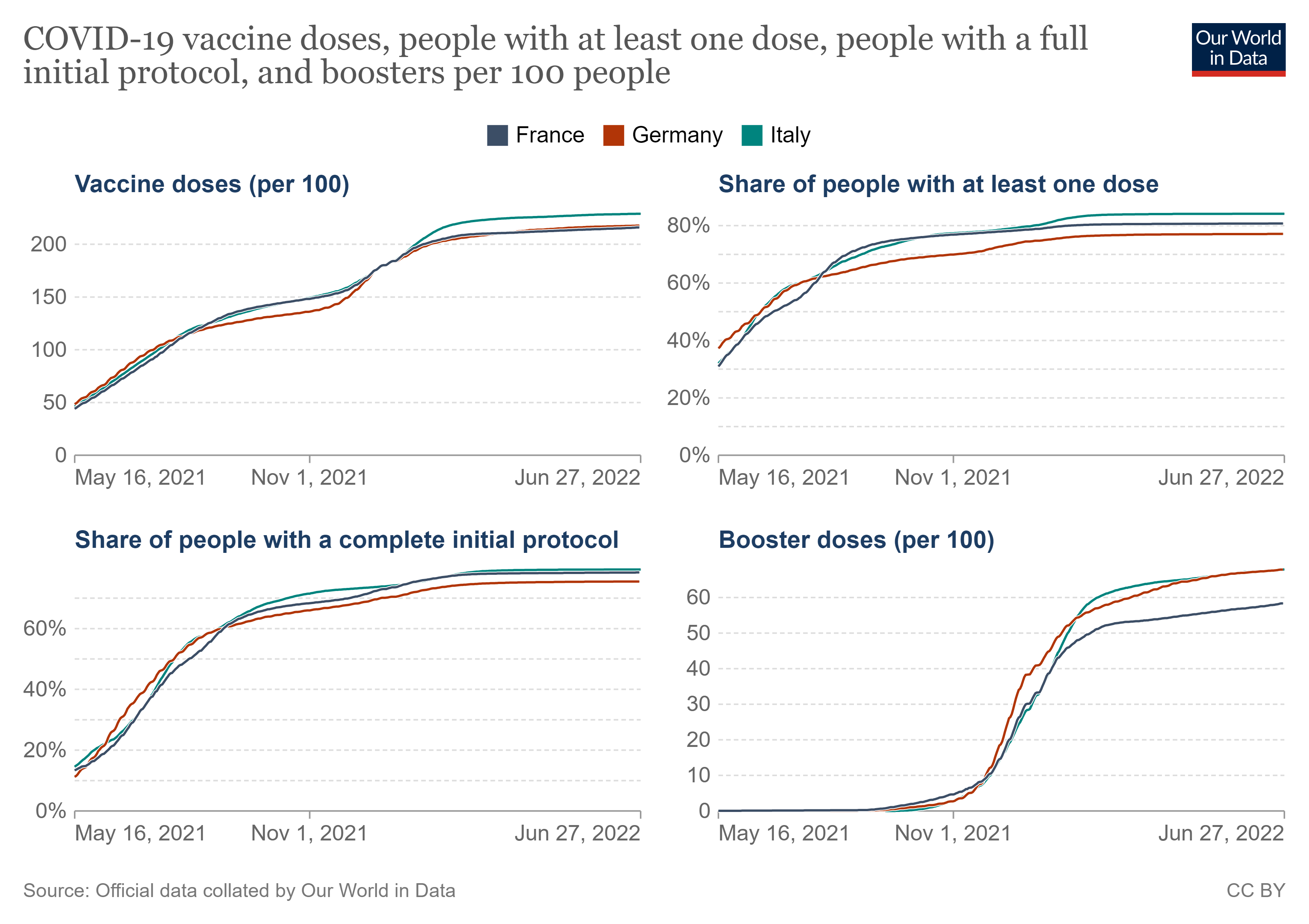
all have similar enough vaxx and boost rates (especially among the old though that is not shown here) that a vaxx signal in one should show up in all.
and spain and UK are in near perfect variant lockstep, one month after portugal.
(the drop in UK is a data artifact, not a real trend)

portugal saw covid deaths start to spike 4 weeks after BA.4-5 hit 10% of cases.
this happened the week of 5/16 in spain and UK, so if this signal is variant interacting with with vaccine, we should be expecting to see it by now.
but we aren’t.
as can be seen, both spain and UK are pancake flat on deaths and basically right on the lows. whatever drove portugal from 2 to 5 deaths per mm per day did not occur in the rest of the iberian peninsula or across the channel.
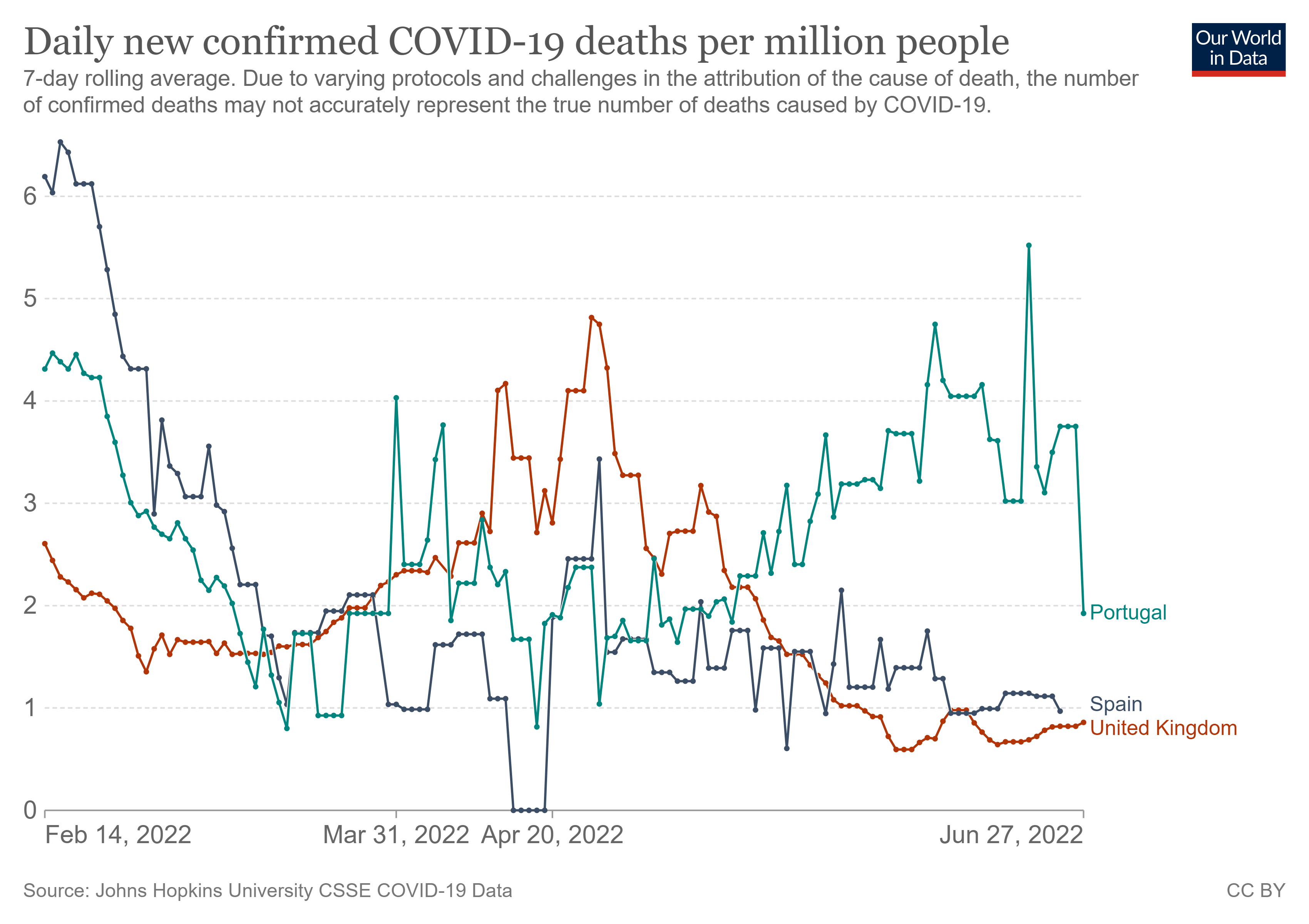
lest i be accused of cherry picking, here is the rest of the neighborhood:
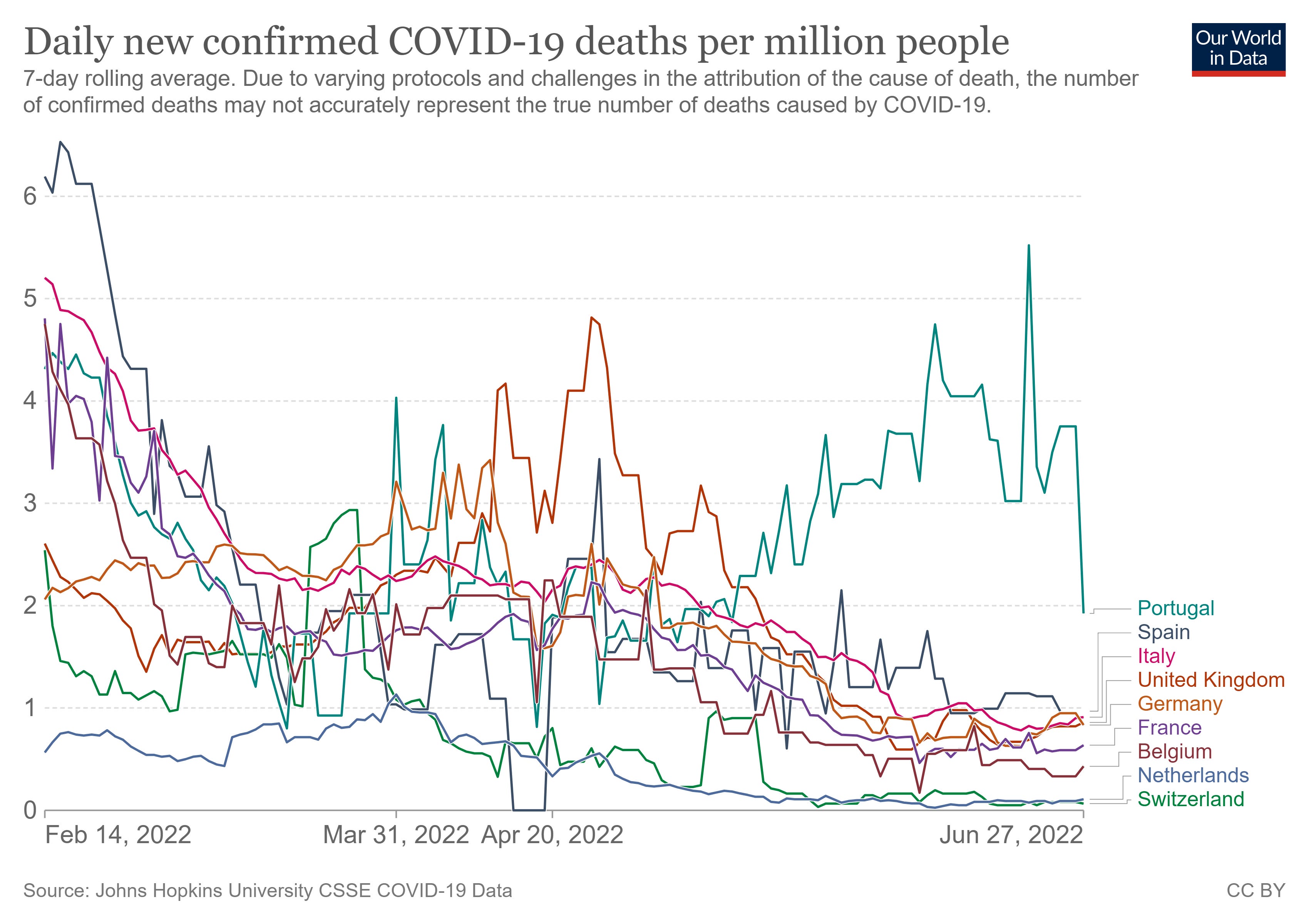
as can be readily seen, portugal looks like an outlier. whatever is going on there seems unlike anything going on anywhere else around them.
this seems to pose some near fatal problems for the “BA.4-5 driving deaths in high vaxx” hypothesis. i suspect we should wait another couple weeks to be sure it’s not just time lag, but at the moment, the odds on assumption seems to be that this hypothesis has been falsified. (hey, that’s science for you and if you’re not trying to actively disprove your theories, you’re doing it wrong)
there was, however, some interesting looking subset data:
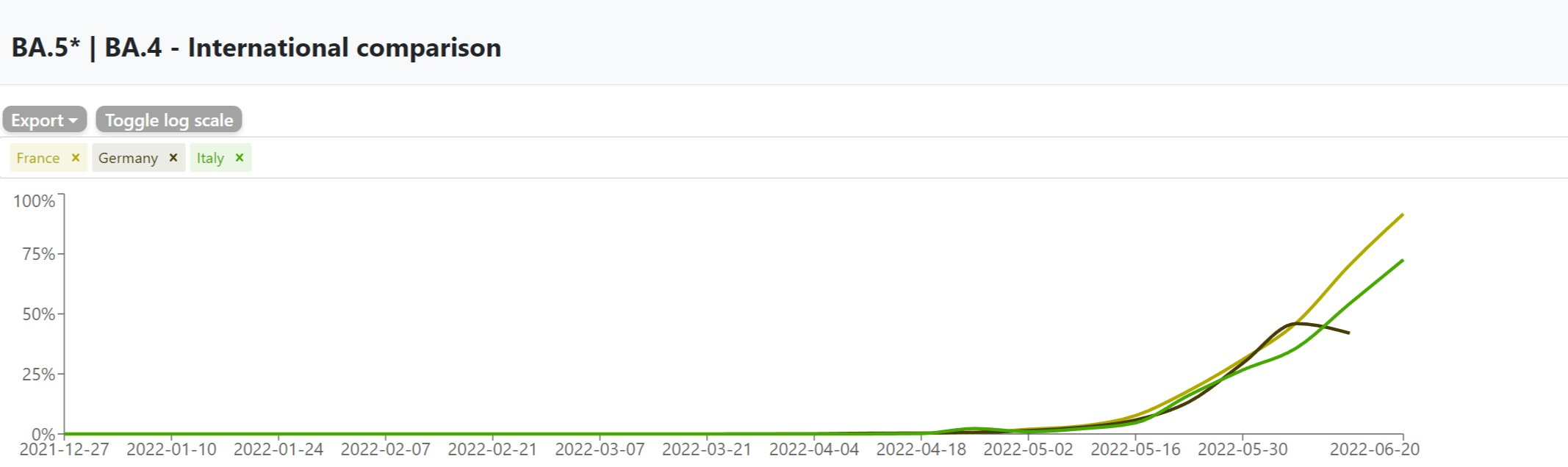
all passed through 10% the week of 5/23 and look to be in tight lockstep.
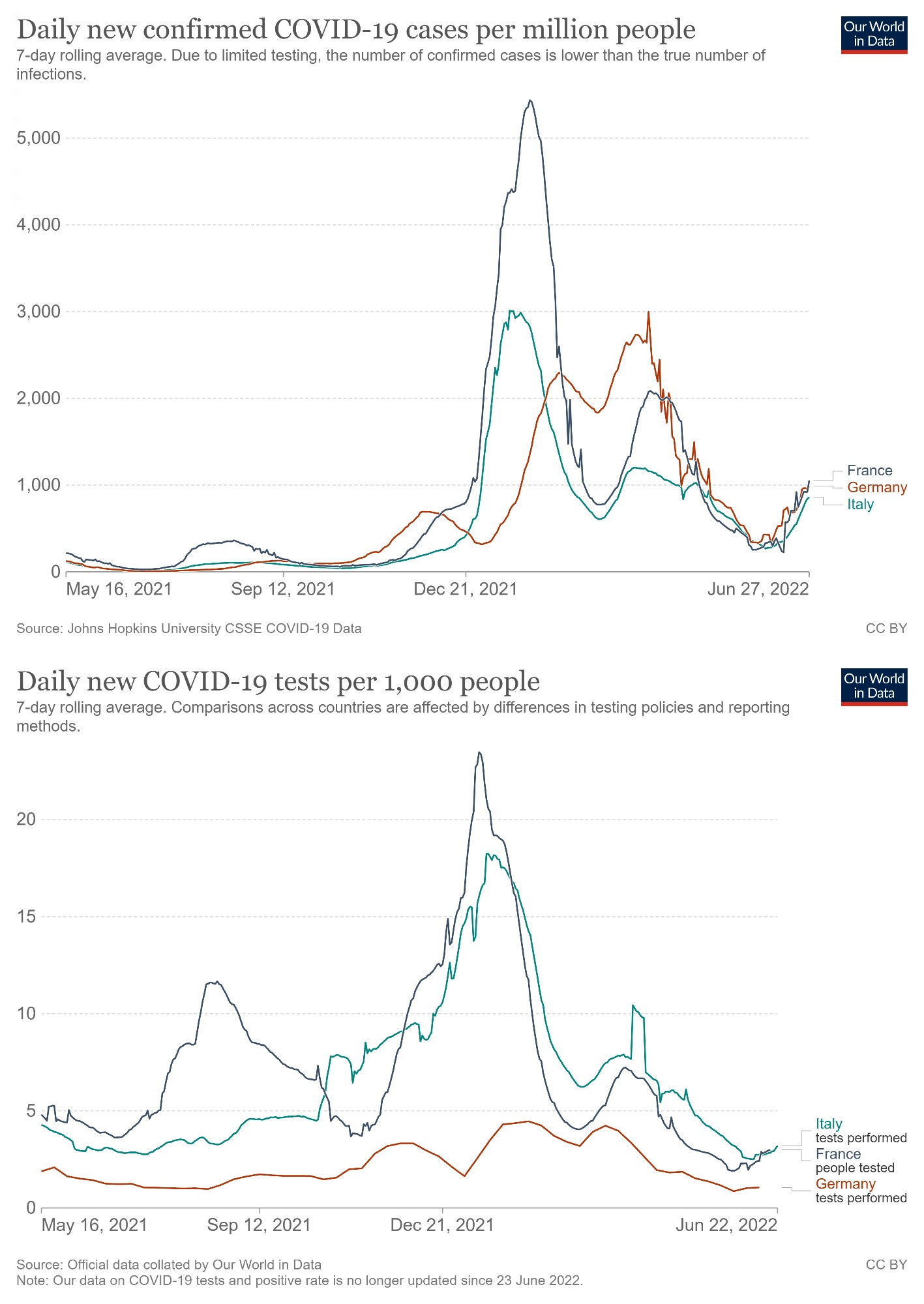
and all are seeing spikes in cases well in excess of anything this time last year despite testing less than this time last year (showing that this is not a sample rate issue but rather an understatement of the rise in prevalence)
this rise coincides tightly with the rise of BA variant prevalence.
this would seem to confirm that the BA variants are, in fact, spreading more despite high levels of vaccination.
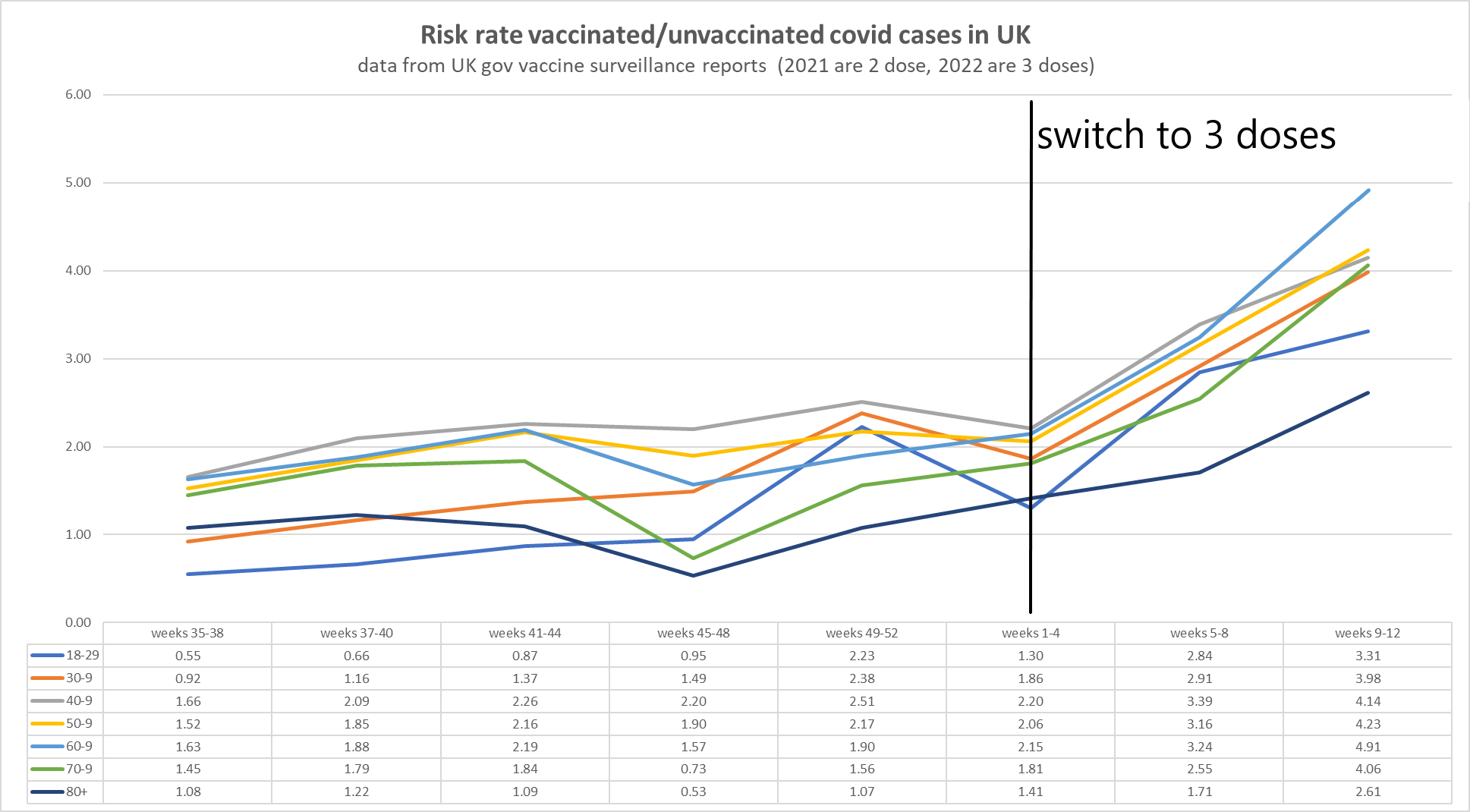
the UK data had been showing us that the vaxxed and boosted were getting covid at 3-4X the rate of the unvaxxed even when we stratify by age, so more vaxx more covid is in no way surprising.
it’s a shame they stopped publishing this report so we cannot see how BA is affecting this result, but i suspect this data was simply getting too awkward to share. once omi hit, cases blew out in in the boosted.
so it looks to me like we’re seeing a classic, expected OAS curve.
genes are selfish. all a virus “wants” is to replicate. covid is adapting to herd antigenic fixation by selecting for variants that spread most readily in the vaccinated. they have become the primary infected and the primary spread vector.
and they seem to be getting covid again and again and failing to generate long term immunity.
spread is rife and waves are tightening and moving increasingly out of season as variants sweep.
this is being counterbalanced by a large drop in severity esp as new variants seem to lack affinity for deep lung infection.
this sets up a tricky equation. a 50% drop in CFR can be canceled out in overall death generation if you have 2X the cases and at 4X, you get twice the deaths.
this seems like the area we need to work on, but the case that this is now predominantly a disease carried and spread by the vaccinated looks strong and that means that it is they and their leaky vaccines that are driving covid evolution.
what would be REALLY interesting to get at would be a sense of just how much more contagious BA really is vs how much of the additional spread is coming from vaccines. has anyone seen any good work or methodological ideas on how to isolate R in the unvaxxed vs the vaxxed?

Subscribe to bad cattitude
come for the cat. stay for the toxoplasmosis.











I will almost certainly be being dumb here, but:
1. How confident can we be about the variants claim? Not “do they really exist as separate, infective species”, but “in this population of people, some of whom get a positive PCR test, how confident are we that they’ve really got variant X & not Y?” I don’t think the PCR tests have been edited such that positive results are only possible if a particular variant is present. They’re surely relying on a 3rd party running full sequencing on a proportion of samples. I’m not sure every country can do this. The greatest capacity for this expertise is in UK, so it may even be the case that public health depts ‘contract out’ to labs in UK that sequencing.
2. In order to determine a case rate, don’t we need to know the number of tests run as well as the conditions of how the tests are run? Yet we rarely see “positive test results per 10,000 tests” or similar or “operational false positive rate was shown to be <0.1%”. I know we’ve come to depend upon the Our World In Data etc, but how many people know that the operators of such databases are the perpetrators themselves? For example, one of the two most-used global databases is Johns Hopkins University, who are lavishly funded by you know who philanthropaths.
Not that any of this is a surprise, I’m outing myself as a total non-believer in the reliability of these data series. They might be being made up as far as I’m concerned!
Thank you, Gato, for your indefatigable work. In asking the above, to be clear, I am not gratuitously throwing doubt on your hypothesis-making. 🤗
Could the difference be because Portugal has BA.5.1 while Spain does not? Take a look here: https://outbreak.info/situation-reports?pango=BA.5.1&selected=PRT&loc=PRT&loc=ESP&overlay=false
Same with South Africa - they had BA.5 but not BA.5.1 like Portugal.
On that same site you can compare BA.5 and BA.5.1. One of the mutations that is different regards: L37F
This study says L37F is associated with more severe outcomes.
https://pubmed.ncbi.nlm.nih.gov/33179934/
I don't know if that mutation is worse for vaccinated, or bad for everyone.