



omicron booster boosterism and the fate of public health
this is not the road to regaining trust

gatopal™ jay asks a simple and astute question here:

and while it’s certainly tempting to respond with something like this

because we have all certainly had just about enough of this:
i think there remains something of a path back if health agencies were willing to follow it, but that is a path of opening the data and making most of public health into something more like a utility than an ivory tower cum bully pulpit.
it’s not at all clear to me that in the information age that we need public health agencies at all when we could instead have networks of data and open analysis easily published, monitored with many eyes with varying perspectives, and spread and with real, adversarial peer review and replication as its underpinning, but were i a current denizen of the public health cathedrals who wanted to have even an agency (much less a job) in 3 years i’d sure be making moves to become open, honest, and forthcoming to well beyond the point of reproach.
unfortunately, nearly all seem to be going the other way.
former head of brown university’s school of public health ashish jha has been increasingly taking over the role of “public covid mouthpiece” for the biden administration of late.
unfortunately (and astonishingly) he seems to have even less grasp on the facts or the data than did folks like fauci, birx, and wallensky.
what he is pushing here is past irrelevant and well into outright presumptive fabrication.
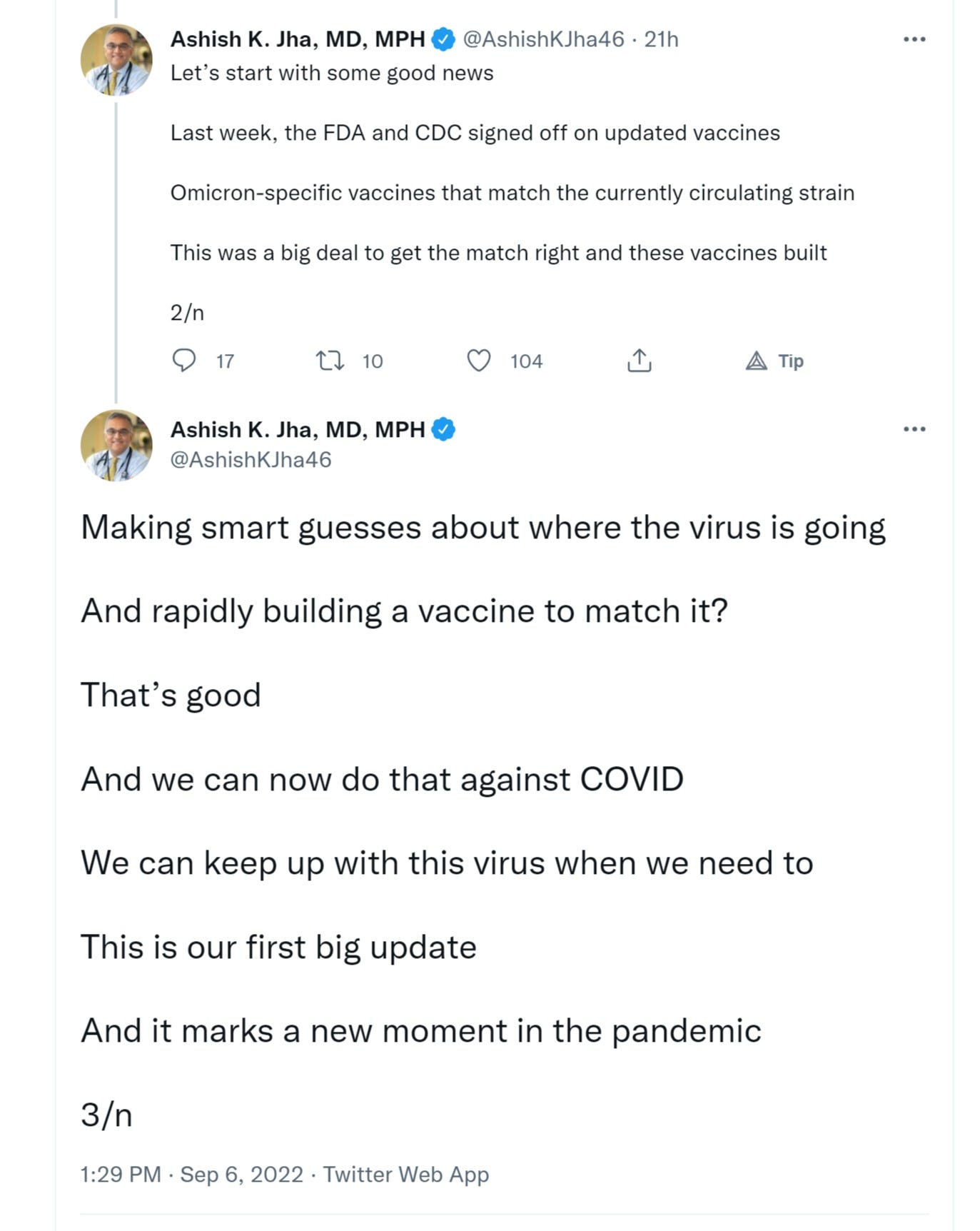
”the FDA and CDC signed off” on “omicron specific vaccines.”
sounds impressive. but is it?
well, no, not really when the data you used to generate “approval” was mouse data.
and it was not even clinical mouse data. it was proxy data.
they gave the vaccine to mice and tested for antibody response. the presumption that the antibodies will work to stop covid is based on nothing whatsoever, just as the booster data was.
and just like the boosters, the FDA did not even allow an expert panel to give an opinion here for fear of what they might say. it appears that not even the FDA “trusts the experts” anymore.
oopsie.
this alone is an entire field of well covered red flags especially in light of the fact that such studies have already been done in primates and showed a stunning propensity to not work. variant specific boosters failed to elicit novel response in the previously vaccinated.
this is a scatter of memory B cell specificities post immunization and boosting. think of B cells as a recipe storage medium. they are not the antibodies, they are the cells that remember which antibodies to make and how to make them. it’s your immune memory.
these charts are a little tricky to read, so let’s walk through them:
the scatters break into 4 quadrants. upper left are B cells specific to the Y axis variant. lower right are B cells specific to the X axis variant. the upper right are effective on both.
look what happens here. you can see fade from week 6 to week 41 and then a resurgence in week 43 (post a week 41 boost)
now look at how different the responses to omi are vs traditional 1273.
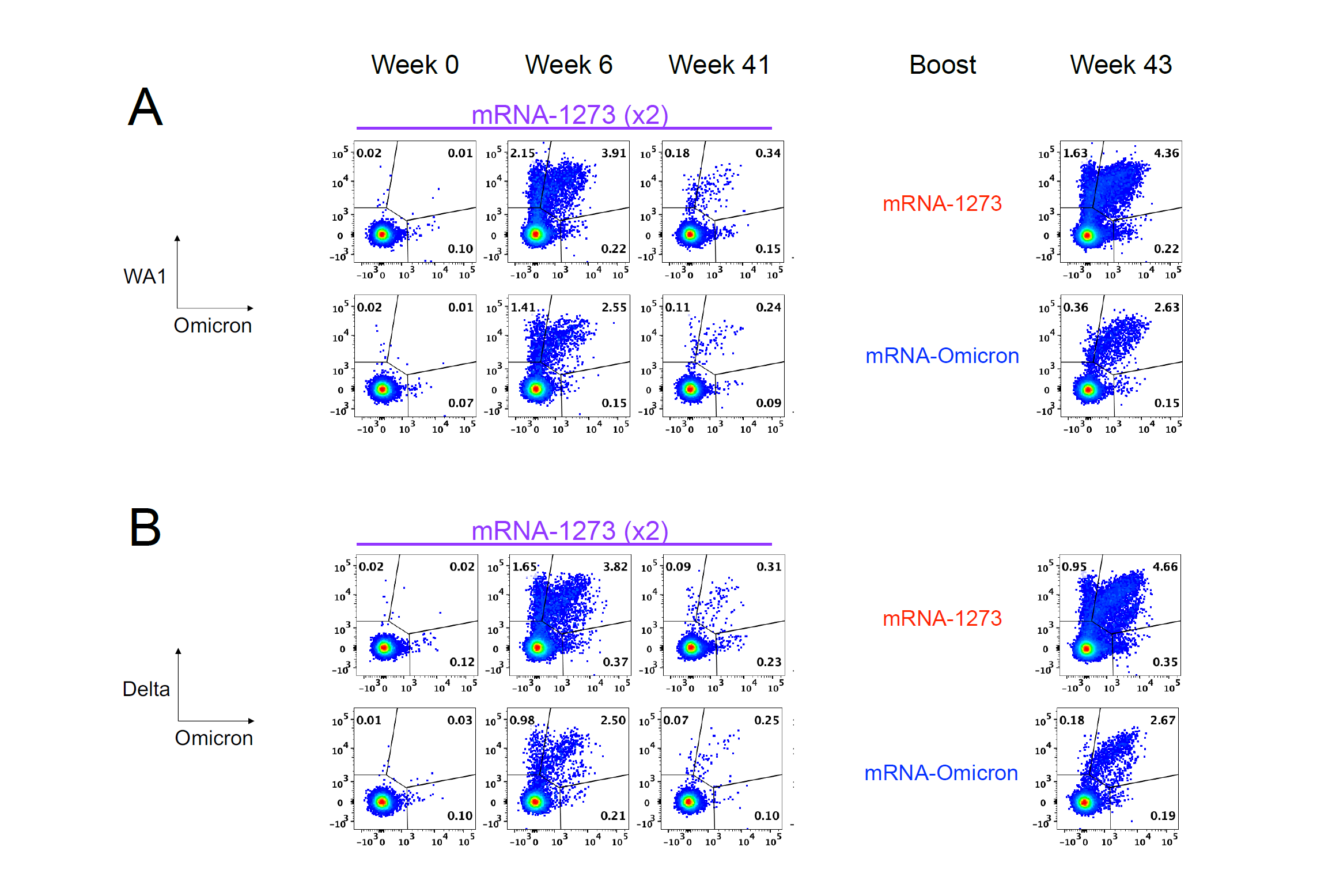
not only is the response more muted, it’s FAR less broad. you’re getting far less B cell variety from the variant based booster, but more tellingly, it’s ALL a subset of the 1273 boost’s elicitations.
there is nothing new.

a new pathogen with more than 30 mutations on the S protein evoked NO new immune response. that is, to say the least, VERY suggestive. one might even go so far as to call it “outright worrying.”
it means your immune response has ceased to be trainable.
so, we have strong, a priori reason to doubt the validity of this purported clinical marker.
one of a more cynical bent might even suspect that the mouse booster™ model was deliberately chosen to mask this issue and overstate efficacy.
i have a serious question on this that i have not seen answered anywhere in the public sphere:
just what was this “antibody proxy” used in the pfizer and moderna trials? what are these “neutralizing titers” because as we saw in the primate studies, variant specific boosters failed to elicit novel response and so i’m curious about just what they used here to claim they saw such an outcome and just how “novel” it turns out to be, especially in the bivalent where 5/8 of mice exhibited titer expression in the same range (or in one case lower) than the original BNT16b2 vaccine.
and if this titer was already present in mice dosed with the original vaccine, isn’t that confirming that it is NOT novel and as we know it’s not only failing clinically vs omi but leading to MORE cases in the vaxxed, on what basis are we to assume that it suddenly “works now because we branded it variant specific”?
not exactly dazzling reasons for faith here, are there?
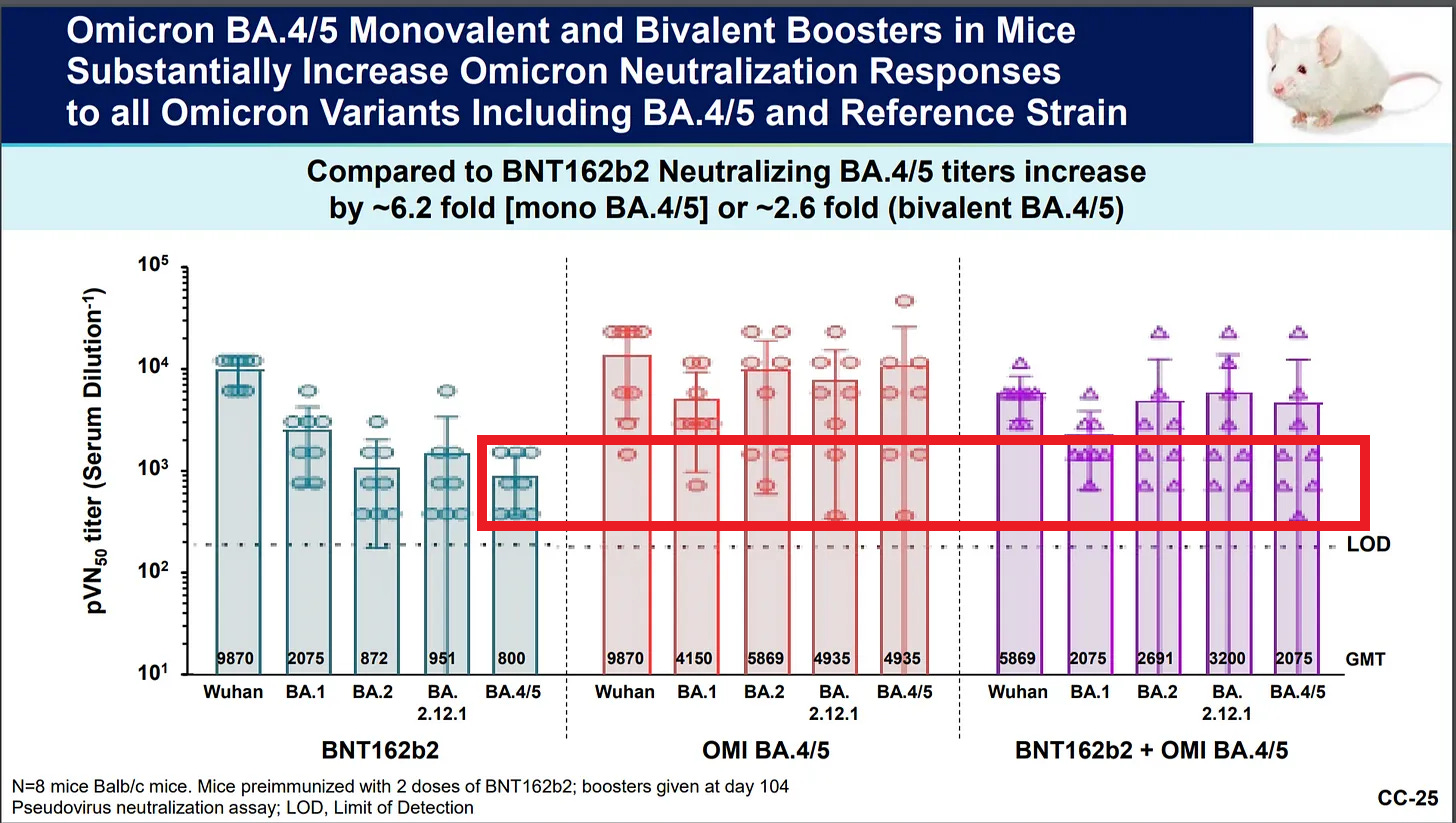
the distribution of the outcomes itself for BA4/5 is suspicious as this is a log scale and the greater than 2 log variance implies more than 100X variation between subjects (8 mice) and eyeballs to more like 500X in the omi ba4/5 solo dose.
that’s awfully wide and makes me wonder about just what they picked. did they basically data-mine post facto looking for what is basically one blue dot from the above scatters and then present it as “evidence of effect”?
the level of variation in response seems awfully odd for a product with a sound efficacy modality. (and it’s 10-50X the variance of the original jab)
pfizer’s proclivities to play “pfast and loose” with the data here have been on vivid display all along.
is this more of the same? i presume the FDA has piles more data here than any of us have seen.
if you want out trust, then release it.
why should ANY of this reside outside the public domain?
and what reason exists to presume this titer maps to clinical outcomes?
a worrying fact pattern emerges from the moderna mouse study where the mice were given a full 3 dose course of the two “original” moderna jabs and the new BA.5 booster.
but then:
All ten mice, vaccinated with Moderna Ba.5 booster, became infected with Covid when challenged with Ba.5 variant virus after receiving their Ba.5-based bivalent boosters!

obviously, that’s not good and casts still further doubt on the idea that these “titers” demonstrate any useful clinical outcome.
this looks less like science than like story time in the marketing department.
many EU nations have banned or contra indicated these vaccines and boosters for young, healthy people. these are not “vaccine deniers” they are “reality accepters” who, having seen the data, are stepping up to say no more.
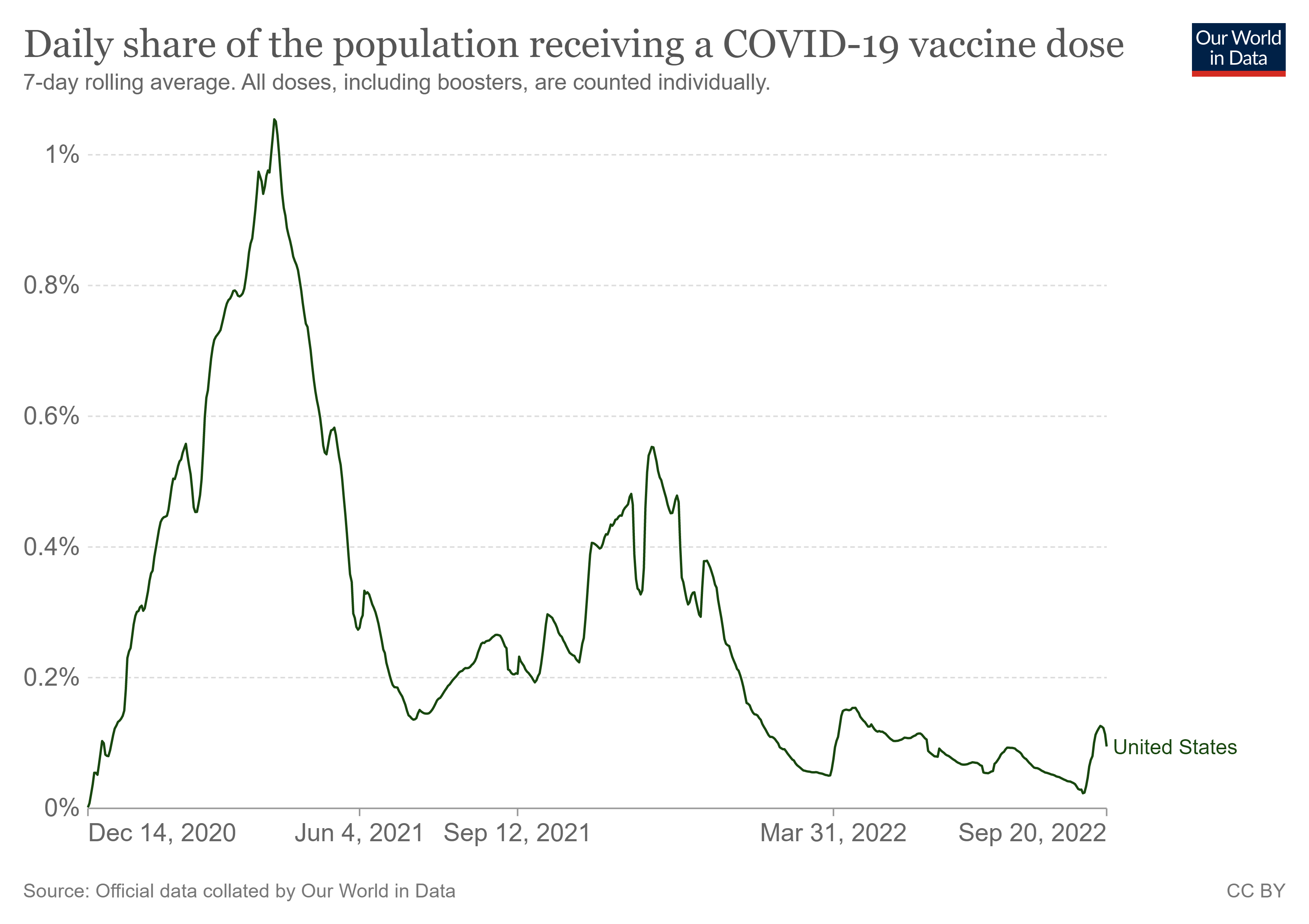
so there are A LOT of reasons to be skeptical of the american public health position here and this skepticism is showing up strongly in the bivalent vaccine uptake data.
only about 1.5% of americans have gotten the bivalent booster.
virtually no children have. because they shouldn’t. and the public knows this now.
public health officials have been so wildly wrong and dishonest all through covid it’s really pretty overwhelming.
and even colleagues and friends who were calling me “the tinfoil cat” early on are now seeing with open eyes just how wrong they were about assumptions of probity and competence in public health. they no longer trust experts either.
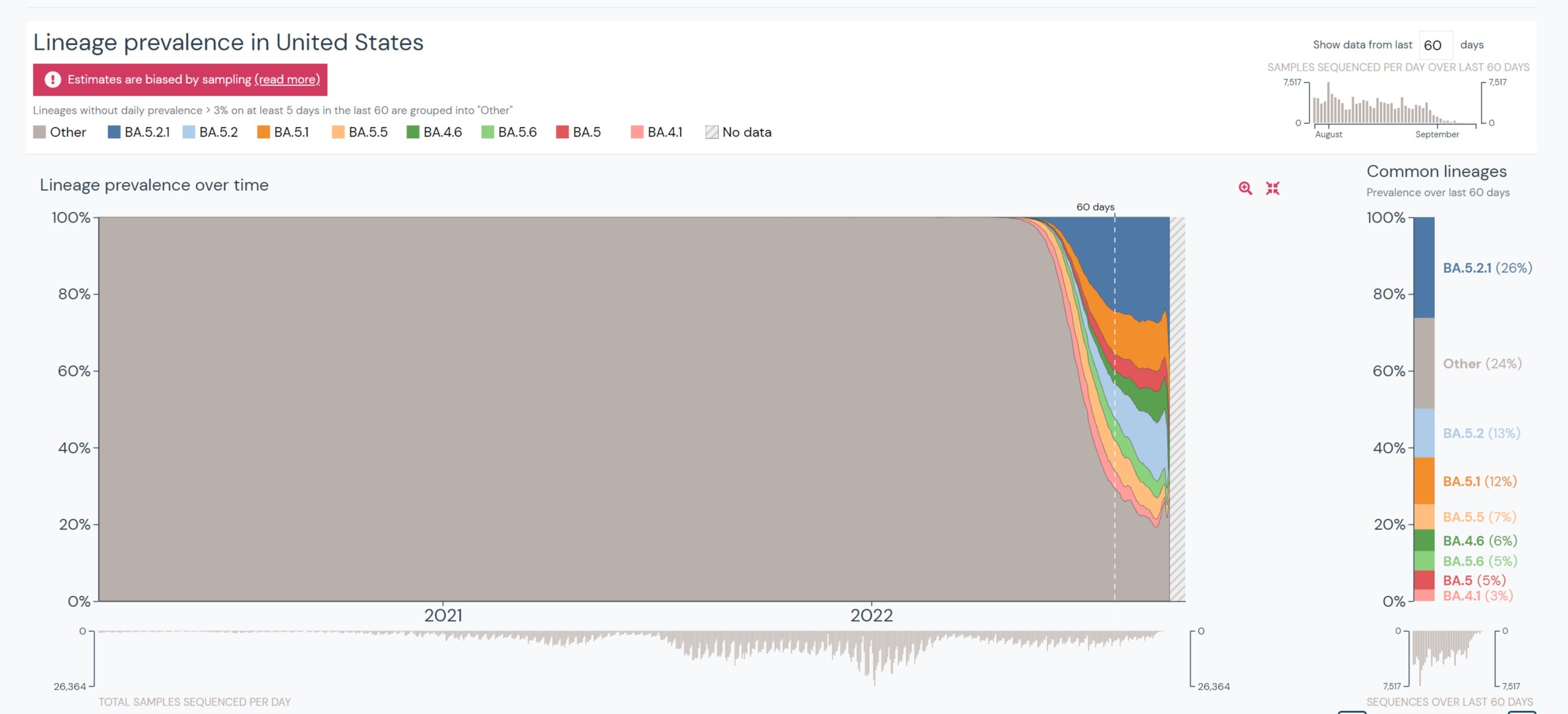
and all this talk of “anticipating new variants” is nonsense. original BA 4/5 are already pretty much gone. this is shooting WAY behind the plane and will be further still off target by peak winter season 3 months from now (especially given the propensity of this virus to evolve to be vaccine advantaged by leaky vaccines).
so what now?
the simple fact is that i do not think there are people who can fix this. there is simply no one you could put in charge of agencies that act like this that would restore confidence and even if there were, who would come next and how could we avoid sliding back down the same slippery slope?
i don’t think we could.
instead, we must change the nature of the agencies, open the data, open the process, and let the sunshine into everything. public health must be made public. ultimately, the need for agencies at all must atrophy and systems emerge to replace top down diktat with agoras of competing data analysis. we can link hospitals and doctors and anonymized data and have a sea of information at our fingertips instead of miserly and inept portioning it out in service of fief building and agenda.
can you imagine any market that would have simply refused to assess VAERS safety signals despite the 120db alarm bells ringing for 2 years as the CDC did and continues to do?
if we would truly serve public health, we need markets, not monopolies.
that will allow us to become our own safety net and to inform and inhabit it.
it’s a system of competition and cooperation not coercion and corruption.
that is really the only system you can trust to keep you safe.












Thank you so much for this thoughtful article, and for all you do to save humanity. I often share your posts, which are extremely interesting and enjoyable to read.
I wanted to share with your readers this compilation https://truth613.substack.com/p/from-my-heart, which attempts to wake up everyone to the global agenda, even those people who think that the covid shots are beneficial. I hoped that by focusing on other aspects of the tyranny, they might come to realize that something is very wrong.
Tonight and Monday-Tuesday is the anniversary of the creation of mankind and a day of judgment for all humanity for the coming year, so it’s a very important time to pray to the One G-d, the Creator, to save us from the evil plans. https://truth613.substack.com/p/inspiration-for-the-new-year
May you and all of us be blessed with a good, sweet year! Shana tova!
"Public health" is just a make work project. Abandon it totally as it is corrupt to the core and redundant. The people who should take care of public health are the public - look after their own health. If there is a rodent infestation in a restaurant, call the exterminators. If there is an outbreak of illness in a city, task a few doctors to figure it out. No need for these health czars with huge salaries and massive pensions.
Where trust needs to be rebuilt is in the medical profession itself.
Shut down the school vax program totally. Clean up the inner cities and support the working poor.