the “swiss cheese” model of covid protection is a matryoshka doll of nested fallacies and statistical illiteracy wrapped up in a zeno’s paradox. this is being spread by media and public health officials alike as though it were some sort of epidemiological strategy for risk mitigation. it is not. it’s deeply ignorant denial of science and data being used as a form of propaganda. even a cursory glance at its underpinnings demonstrates this.
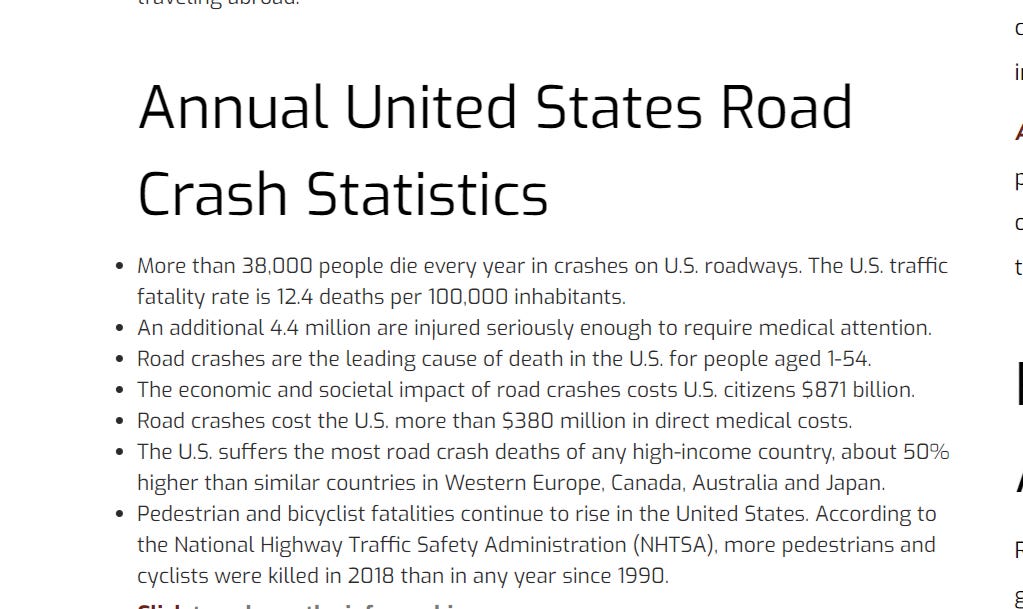
cliff notes: you have about a 0.9% lifetime chance of dying in a car crash in the US. your risk of getting covid post vaccination and then dying from it is on the order of 0.015% even if we add no other mitigations and assume you have a 100% chance of getting covid without a vaccine. this is 1/78th the risk of death by car crash over a lifetime.
most americans are OK with this car risk. we drive and we speed. almost none would accept a driving ban or a 30 MPH speed limit on highways to drop this risk by half or to push “zero car deaths.” so what is the case for doing 100X that economic and social damage to reduce covid risk or push “zero covid”? the whole argument is rooted in fallacy and fear mongering.
swiss cheese is hallucinatory fear based delusion masquerading as public health.
the question was never “how do we reach zero covid?”
the question was always “would i pull my kid of out school for a year to drop their lifetime chance or dying in a car crash by less than 0.0001?”
examining the cheese:
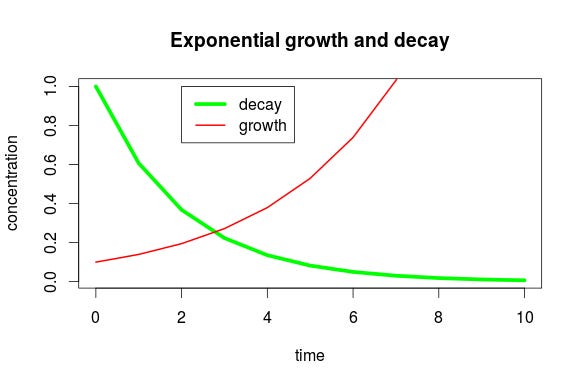
first off, this strategy starts with the outlandish “zero covid” idea as though such a thing were even possible. it’s not. it is a literal mathematical impossibility. there is still influenza from 1918 kicking around somewhere. this is just ZENO’S PARADOX where you get halfway there and halfway from there and so on but never arrive. if you make bacon in your kitchen today, you can clean it again and again and you can never get all the bacon trace out. ever. if you spent a million dollars and had the room cleaned by the people who build semiconductor fabs, you could not eradicate the last molecule of pork. no one can. nothing can be made 100% safe or 100% eliminated and the price for each subsequent halving rises exponentially while benefit shrinks the same way.
pretty soon, you’re paying a trillion dollars to buy nothing anyone can even detect. it’s a ludicrous standard and there is not a single thing in human life that gets handled that way.
taking a shower does not have a zero risk of death. you’d be safer if you wore a helmet and maybe a harness while you shower. do you? i’m guessing no. why not? because taking a shower is, for most people, very safe. the risk is so low, that even reducing it by 50% is not worth the trouble.
if i could sell you an “anti-meteor hat” that really, provably reduced your chance of being hit by a meteorite by 90%, how much would you pay? would you even be willing to wear it all the time if i gave it to you for free but it was even slightly uncomfortable or unfashionable? i doubt it. why?
because a 90% reduction of a risk already that low is not worth anything.
that’s the key concept here.
let’s now explore how this fits with covid.
this claim has been widely made (including by the US surgeon general)
the argument is that vaccines, despite what was promised, are not enough for you to get your life back. there is no “normal” just a “new normal” of constant distancing and masking and vigilance. they then go on to explicitly invoke 100% as a standard.
but as discussed above, 100% is an impossible outcome and as we approach it asymptotically, the benefit of each additional mitigation drops exponentially. a 50% drop from 10% likelihood is 5%. we might find that relevant. a 50% drop from 1% is only 0.5%. from 0.1%, well, now we’re only dropping 1/20th of 1% and passing any sort of cost/benefit test is going to get A LOT harder.
so let’s look at where we are by setting up some standards. to start, i am not going to accept “getting a mild flu-like illness” as some massive risk. we’ve lived with flu for 1000’s of years and we take little care to avoid it. we do not distance, mask, or lockdown. we stay home when we are sick and we (maybe) wash our hands a bit more during flu season.
the human race has long since expressed its clear risk preference on flu like illness and it seems to be the only reasonable and fair baseline to use.
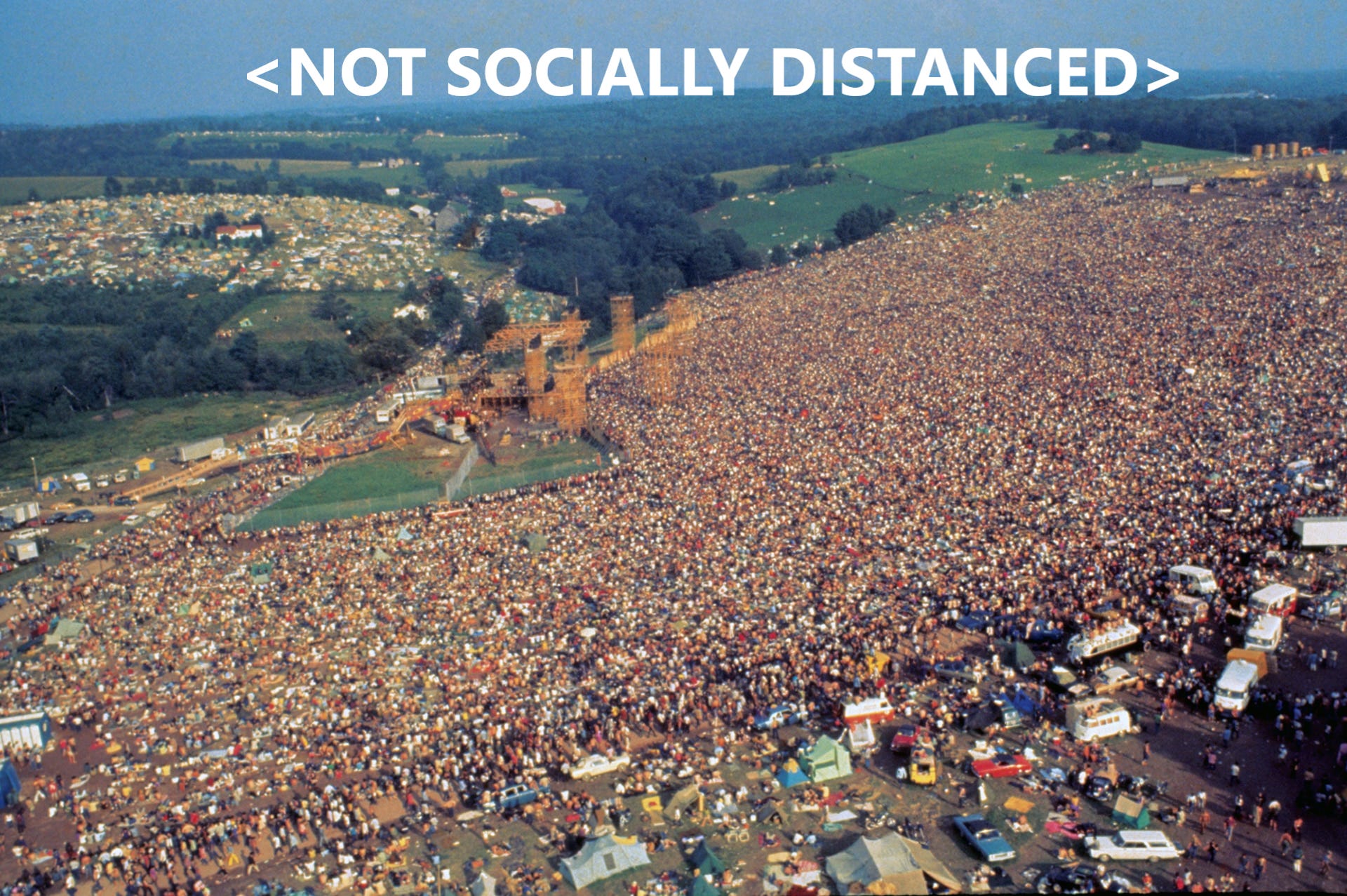
the 1968-9 flu (hong kong flu) was, in population adjusted terms, worse than covid 19 on deaths. ask your parents/grandparents if they even remember it. they certainly did not cower from it or lock down. that was the year that woodstock took place. during a “pandemic” worse than this one.
so let’s look at covid risk:
the global IFR looks to be about 0.15%. john ionnidas, who has been among the best on this, set the number. you can see discussion HERE.
we can then look at attack rate from covid. what is your chance of getting it? so long as you are not around people who actually have symptoms, it’s vanishingly low even if you share a home with them/sleep in the same bed. it’s 0.7% and that is for prolonged exposure and shared facilities/bathroom/food/etc. you can see discussion of that study HERE.
so, if we take as our risk standard 0.15% X 0.7% from high exposure to asymptomatics, we’re at 0.00105%. (1 in 95,000)
if we take the upper risk bound of 18% spread from symptomatic carriers, it’s 0.027%. (1 in 3,703)
so let’s call this a basic risk window against which to start to consider covid risk.
if you are young, healthy and avoid actually cohabitating with sick people your risk is likely 1/10th to 1/100th the lower bound. so you’re getting into the 1 in a million-one in 10 million range.
for you, even taking a vaccine would need to be almost perfectly safe to outweigh the miniscule benefit it even COULD provide you. far from being an irrational choice, it might well be the clear and obvious personal risk minimizing choice to NOT take an experimental vaccine.
the idea of being forced to vaccinate mitigate a risk far lower than death by bee sting seems outlandish.
if you are obese, diabetic, or posses some other set of risk factors, perhaps this looks very different and the vaccine benefit far outweighs the risks. (ask your trusted medical advisor. i am not looking to give anyone medical advice here.)
but maybe others must live in fear of you as a carrier. that seems to be a popular narrative.
so let’s look at vaccines:
now let’s consider a vaccine that is, say 90% effective at preventing covid infection. (many make higher claims, but let’s be conservative)
this drops the high risk case from living with a symptomatic carrier to 1 in 37,030.
it drops the low risk case from living with an asymptomatic carrier to 1 in 950,000
it drops the risk from passing someone on the street or in the grocery store to something far lower. we’re getting into absolutely negligible territory.
so what is there left for masks to even work on? if i am asymptomatic and shop near you, my chance of spreading disease to you is easily less than 0.7%. that would be for living with you, sharing food, furniture, bathrooms, and possibly a bed. i have no reliable stats on how much lower, but 10-100x is likely the correct magnitude.
this takes us into the truly infinitesimal ranges of 1 in 10 million of so, possibly 1 in 100 million.
the idea that i owe it to you to limit my life to change your outcomes by less than the chance of getting struck by lightning is a preposterous moral inversion even if these mitigations are REALLY effective (and they aren’t.) your base risk is so low that nothing i do can affect it in any manner that humans have ever been shown to care about in any other circumstance even when we pile this all up.
chances of dying from a car crash in the US are 124 in a million per person per year. 14,357 per year need medical attention. this death toll is rising. we keep driving faster.
if we could drop it by 70% by dropping the speed limit on highways to 30 mph and enforcing it utterly, would you vote in favor? would it be worth the social or economic price? because i sure do not see any remotely representative groups with even a modicum of public support stepping up and making a case for it. most people i know want speed limits raised. most people i know exceed current limits almost every time they drive. it looks to me like this is a level of risk american humans find acceptable/desirable.
124 per million per year die via automobile. 14,357 per million need medical care. that’s the roads.
covid risk of death if you are vaccinated even if you live with a symptomatic person looks to be on the order of 27 per million.
for asymptomatic, it’s 1 per million and unlike driving, this is a one time risk as getting covid a second time is vashishingly rare, cars are a risk every year and thus that risk is cumulative.
over a lifetime of, say, 80 years, that 0.124% nets out to a ~0.9% chance of dying in a car.
let’s then compare that to the risk of 0.15% IFR X 10% (contraction risk based on 90% success rate on a vaccine).
that’s 0.015%. 1/60th the chance you’ll die in a car crash over your lifetime.
even if you got covid twice, it’s 1/30th. and this assumes you had a 100% chance of getting covid if you were unvaxxed. we can compare covid deaths to lifetime risks for this reason. your risk is really just once a lifetime and these mitigations are costs that could last a lifetime if we keep going as we are.
so just what are we playing at here with all this “swiss cheese”? there is flat out nothing for it to work on if someone is vaccinated and this is not even taking in to account the fact that IFR is going to plummet as we learn more and have already learned more about treatment. how much IFR is just the result of terrible early policies to push sick people into nursing homes and the early, aggressive ventilator use that proved so fatal?
this simple TREATMENT with a safe, affordable asthma drug might well lop a whole zero off the IFR (it reduced need to seek urgent care by 80-90% in a controlled study) why would anyone even consider another odious or high cost mitigation vs buying people $55 inhalers? (and yes, masking is both odious and poses real health risks. see HERE.
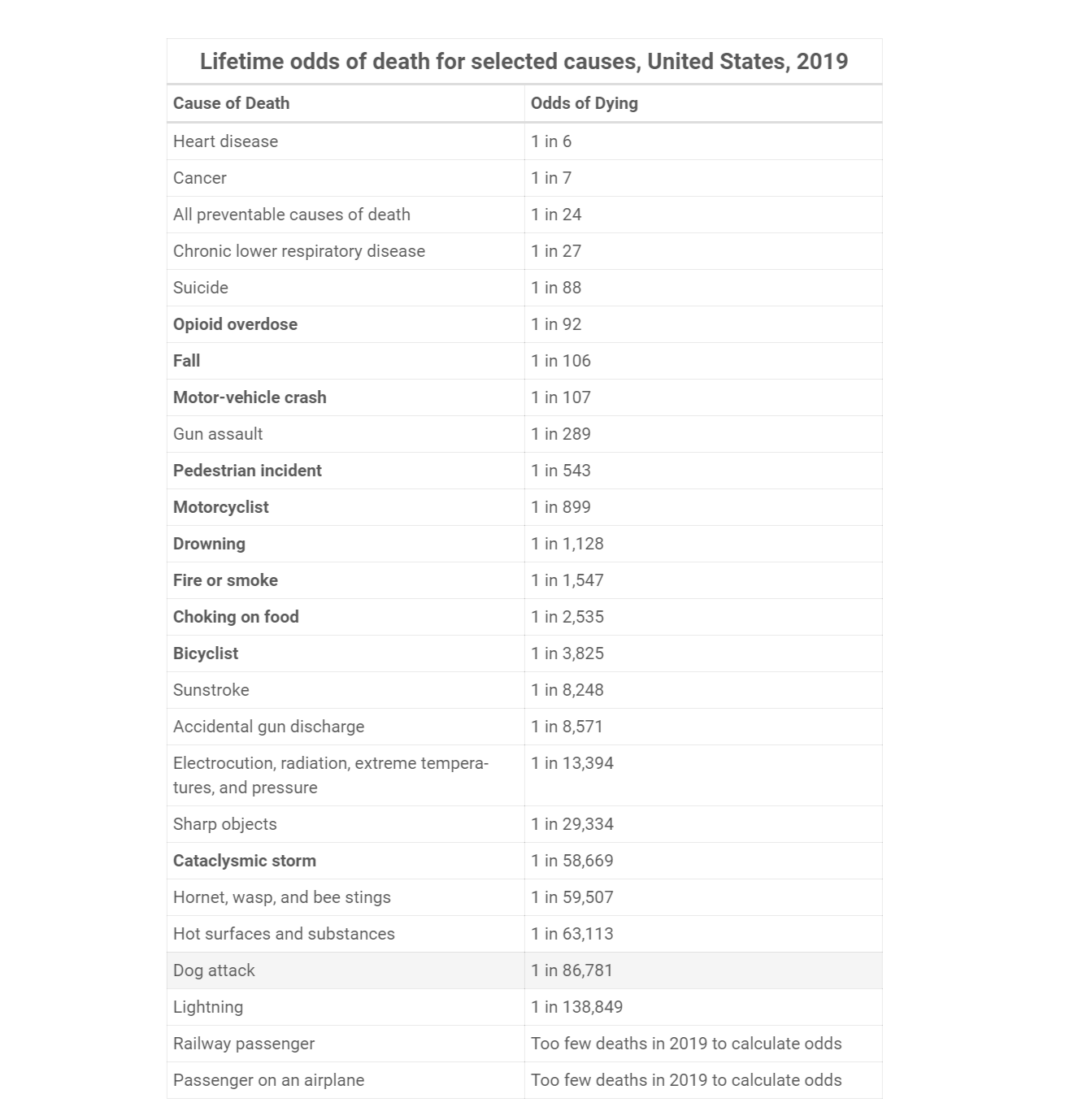
we’re already WAY below risk levels that humans clearly find acceptable and dropping them a further 80-90% looks trivial. death as a vaccinated individual looks to average about 1 in 6,667 (and that’s being highly conservative). this is roughly in line with “death by sunstroke” and roughly 6X “death by drowning.” for the young and healthy, it’s like more like “death by insect stings” and we have not even yet factored in the extremely high likelihood that vaccination would make a later infection milder and thus drop IFR further still. assuming it cuts it by half, we’re at about the level of “electrocution.” SOURCE
so, put their fear and wild claims aside and think rationally: the correct framing for a vaccinated person of average risk is:
“if the mitigation you recommend is 50% effective, it will reduce my risk by about 1/2 my risk of death from sunstroke or 1/30th my risk of dying in a car crash even if i use extremely adverse assumptions.
would i be willing to pay whatever price this is to get that benefit and is there any moral or utilitarian basis whatsoever to force others to pay large costs to get me these infinitesimal or possibly illusory benefits?”
any honest, rational person must answer those questions before even seeking to DISCUSS whether mitigations work (and the data there is pretty terrible). most, including masks and lockdowns, do nothing that is even measurable.
so let’s stop all this absolutist safety theater. it never made sense and no reasonable health official with an even rudimentary grasp of risk factors and cost benefit, the literal bedrock of public heath decision making, could possibly be pushing a vax then mask and distance policy for any but the very highest risk tranches.
this is not medical policy, it’s political propaganda and these sorts of 100% demands are a dead giveaway. this is the truly big lie to push you over the line into trading all your freedom for the illusion of safety from a bugbear conjured into being for just that purpose.
just say no. the society you save may be your own. you do NOT want to see where this is GOING if you don’t.
the bad cat misses twitter as well but after getting cancelled and even seeing good kittens suffer the same fate, i have real doubts that the bullying bluebird has any plans to change it's gato policy. they have refused to even respond to appeals or questions. nothing but silence.
Excellent post. But they will never willingly let us out of this dystopia. Covid cult coordinated talking point this week, by Gates, Fauci, Schwab, BoJo and the CDC lady, says that vaccines " can't get us to zero so we have to keep masking up." Under no circumstances will this bio-fascism be relinquished. None. No logic or data or facts matter here. This is an NGO-mediated cult, and cults are impervious to logic and data. Only organized revolt will stop them.
Great article, great opinion, thx! I notice now that the next straw the 'but it is really really bad!' convicted hold on to, is 'long covid', it is irresponsible to let people get ill at all, at any cost, because the long covid is so common...
Do you have an opinion on that?
First, I think the numbers for it are highly exaggerated.
Second, the 'syndrome' is partially psychosomatic: so much fear for the virus (most sneeze a bit for a few days), that to have the deadly virus is devastating; overlaps with ME, lyme and other (self diagnosed) hard to diagnose (and treat) similar conditions; UK post-vaccination indicates recovery of long-covid-ers (hard to explain physiologically), and some also do test negative.
i have seen literally zero evidence that long covid is any more common, significant, or dangerous than long flu or long pneumonia. any respiratory disease can cause lasting effects. but the definitions being used for "long covid" like "difficulty concentrating" or "low energy" overlap so much with depression that finding any meaningful number in a self reporting study is all but impossible.
you can see how clownish some of these claims are here:
The long-COVID brigade seems to have dispensed with the requirement to demonstrate a positive Covid test at any stage now. So presumably most reports are genuine symptoms but arising from prolonged fear and stress from pro-lockdown psychological manipulation and general fear propaganda. And maybe just wearing masks...
Indeed, the symptoms are real - even if psychosomatic - and need their own treatment, but as you infer, the cause needs to be clear to have a sound evaluation on what measures are appropriate and proportional. The long-covid-ers are genuine - from their perspective - but...? What happened to or is lacking from our scholing system - some critical thinking and statistics for everyone?
of interest, the google search prevalence for terms like "fibromyalgia" and "chronic fatigue syndrome" dropped sharply right when searched for "long covid" spiked. this is supportive of the idea that a subset of people with vague or generalized persistent symptoms simply jumped from one explanation to another.
Zeno paradox argues against the vaccine, ultimately only solitary confinement would be accepted.
The answer to long covid is its: low prevalence, short duration and image/accuracy of diagnosis.
That said prevalence of vaccine long term effects that look like long covid and worse would have Zeno accolades argue against vaccine.......
Vaccine after all causes immune response are similar to the infection! That is you could get all the effects as well as the autoimmune issues!
Also we have variants and the innuendo that corona virus is vastly mutating like flus, which is not implied by low prevalence in corona cold societies..
...as an aside, the vaccine hucksters have *already* announced the need for "booster" shots. Pfizer promised, yesterday I believe, that theirs would be ready by end of 2021. Ooh, that cash is already being counted!
The mRNA vax causes your body to create antibodies against the spike protein the mRNA causes your cells to put on their surfaces. Those antibodies are made by your immune system. What Pfizer is implying: your immune systems forgets, which is not seen in natural immunity that impacts your immune system in a similar manner.
I think we see a permanent vaccine "cold war" like the military industry complex profits from.
Actually, I misspoke. What Pfizer said was, they would have shots that would protect against the (apparently many) variants by end of the year. One could argue that is not a "booster shot" but, in fact, a message to a create antibodies to a different spike protein? That said, I agree with you, IFAIK, natural immunity takes such variants into account. I guess the jury is still out on if an mRNA "vaccine" does the same thing. Not that I believe in conspiracy theories, but it would be more profitable if either: the vaccines did not; or you could convince people that the vaccines did not!
Yes, perpetual pandemic is as good a business model as Lockheed's for the perpetual war threats. Good, solid profits when US buys 100's of billions and shields liability.
I don't agree with your view that "anyone under 60 in good health should not vax". I oppose mandated vaccination, but there's (at minimum) a significant part of that population for which I see a clearly positive cost-benefit.
I sat down last summer and worked out a range of quantification of COVID risk for my own demographic (healthy mid-40's). I had CDC reported COVID fatality data through that point in time (end of July), which included ~157k reported COVID deaths. To get around the denominator issue (actual number of infections), I used a range of assumed overall U.S. IFR's from 0.25% to 1.00%. (I'm aware of Ioannidas' estimate of 0.15% global IFR. The U.S. population is significantly older than the global average, so it's reasonable that U.S. IFR would differ from global.)
I also had CDC data that allowed me to look at reported COVID deaths and cases for ages 40-49 as either "with known underlying conditions" or not". (Important note: I am *not* at any point using a case fatality rate as a measure of risk. I use population-wide IFR's as the measure of fatality risk, but work with relative death / case #'s to try to determine relative risk if a person does or doesn't have an underlying condition.)
With these proportions - plus U.S. demographics by age group - one can adjust to get a view of fatality risk *if contracting COVID* (i.e., an IFR for an age range, with or without underlying conditions). My conclusion was that COVID IFR for a person who is healthy and mid-40's ranges between about 0.039% and 0.156%. At the lower number, that's 1 death per ~2,600 infections. That's fatality risk equivalent to ~3 years of U.S. population-wide risk of vehicle accident fatality. (The higher end of that IFR range is equivalent to ~12 years of vehicle accident fatality risk.)
There are of course bad outcomes - such as being hospitalized for several days, which is no fun - short of death. That can happen with either COVID or a traffic accident, so for simplicity I've assumed those are roughly equal.
(BTW, my conclusion at the time was that COVID was something about which to take some modest precautions, but that I shouldn't fundamentally change how I lived my life. That's for personal risk. Trying not to expose older individuals such as parents was an additional consideration beyond personal well-being, however.)
Now, that risk is of course conditional on getting enough exposure to SARS-CoV-2 to be infected. I would argue that's pretty much an inevitability if everyone under 60 takes Ed's advice and completely avoids vaccination. My assessment is that the risk of a severe outcome from the vaccine - meaning enough to require hospitalization, so not even fatality - is most likely at least a couple orders of magnitude lower (1 in hundreds of thousands). That risk isn't fully known even after clinical trials, but 100+ million people globally have now received the two mRNA vaccines (Pfizer/BioNTech and Moderna). If I could hypothetically get a similar vaccine that would make me essentially immune to traffic accident risk for the next 30,000 (or perhaps more) miles that I drive, I'd do so without hesitation.
I see a lot of the usual arguable points. I do not usually respond to gish gallops.
As of 19 Apr 2021, .09 of US has shown up as "cases" on worldometer. That is 9% prevalence in 14 months, since last June massive numbers (405M) non random testing of mostly asymptomatic subjects.
Risk is plotted P of consequences vs deleterious effects of consequences. P on X axis consequence on the Y.
My observation is under 60 healthy take the 9% chance of the infection rather than 99% (in risk 100% is a casualty not a risk) chance of effects of foreign DNA/mRNA wandering around your cells, induced protein synthesis, and B/T cell effects that last forever.
My personal risk chart said nah! I am over 70 and healthy, I took the vaccine in the AZN trail bc they needed older subjects, science!
I do not have as long to live with my choice as a 60 yo!
"Cases" are known to understate actual infections, though nobody is sure of the exact magntude). Actual cumulative prevalence has been more than 9% in 14 months.
That's why case fatality rate (CFR) is a basically useless stat. That's why there's been so much debate about actual IFR's: nobody *knows* the correct denominator.
Ionnaidis (and others) estimate IFR by trying to find estimates of true infection numbers. Typically those are serology surveys that sample populations for antibodies in order to estimate true infections. (Perhaps those are adjusted for sampling bias, or used as guides to extrapolate more generally about the relationship between actual infections, case counts, and test positivity.)
And here's the key - if estimate of cumulative prevalence to date drops, then implied IFR increases. Assumed U.S. population-wide IFR's of 0.25% to 1% imply ~50 million to ~200 million actual infections, not the ~30 million number Ed's citing (cases).
In other words, if only 9% of the U.S. population has actually been infected to date - which is wildly unlikely, nobody looking at testing details thinks that tests have identified anything like ~100% of actual infections - then you don't want to get it as a healthy mid-40's person because you'd have about 1 in 400 chance of dying if you did.
Another piece of the calculation (which I don't know how to estimate) is that the population that has made it thus far (~ 1 year) without getting sick is presumably less at-risk than average.
At this point, the early treatment discussions are another big tell for me that COVID public health is about totalitarian control and nothing else. You mentioned budesonide, do you have an opinion about ivermectin? It too seems effective but there's a massive noise machine against the signal.
The two biggest risk factors that I can find (after age, which you can do nothing about), are obesity and vitamin D deficiency. How much better off would we have been if government had "mandated" an hour-long walk in the sunshine on days it was possible?
Of course, that wouldn't have the side effects of swinging an election or trillions of printed dollars raining down on the well-connected.
The Cleveland Clinic COVID-19 hospitalization calculator https://riskcalc.org/COVID19Hospitalization/ shows a 3.5% hospitalization risk for a 62 yo white male at an obese 30 BMI and a double 7.2% risk at a thin 20 BMI. They are saying being obese is much better! Follow the science!
you get into too many comparrison instead of making 1 strong one. i preffer the car + shower. and pump up the numbers to 95% .. even with that type of prevention people WILL NOT TAKE the measures
PS. why is the swiss chese image in the thumbnail but not in the article?
i feel like you are too wordy, your points lose their punch with too many words and not simplifying enough.
take "cliff notes: you have about a 0.9% lifetime chance of dying in a car crash in the US. your risk of getting covid post vaccination and then dying from it is on the order of 0.015% even if we add no other mitigations and assume you have a 100% chance of getting covid without a vaccine. this is 1/78th the risk of death by car crash over a lifetime."
vs "cliff notes: you have about a 0.9% lifetime chance of dying in a car crash in the US. assume you have a 100% chance of getting covid without a vaccine. this is 1/78th the risk of death by car crash over a lifetime.
freshman in college in Fall 1968. no memories but we had Vietnam every evening on the 30 minutes national news. LBJ ran on no mushroom clouds in the background. Public health propaganda was not needed in the 1968 election. Not that I made time to see Huntley/Brinkley!
As a 70 year old with low BMI, regular exercise, low blood sugar and on Vit d for years I took the vaccine, largely because I live with a 72 yo who hates Trump! And thinks .00007 risk is too high!
Absolutely fantastic post. My fear is the inability or, in some cases, unwillingness of the populace to appropriately gauge risk will only further embolden health and government officials to continue this safety theatre charade indefinitely.
In any event, thank you for these posts. It is comforting to know critical thinking isn’t completely dead.
The shorthand way of looking at what’s been imposed in the name of covid protection is, Would you shoot yourself or your children in the head (or abdomen or leg) to reduce the chance of dying from another gunshot or some other everyday event?





I miss the cat on Twitter but really enjoy these posts that are able to go into depth.
the bad cat misses twitter as well but after getting cancelled and even seeing good kittens suffer the same fate, i have real doubts that the bullying bluebird has any plans to change it's gato policy. they have refused to even respond to appeals or questions. nothing but silence.
Excellent post. But they will never willingly let us out of this dystopia. Covid cult coordinated talking point this week, by Gates, Fauci, Schwab, BoJo and the CDC lady, says that vaccines " can't get us to zero so we have to keep masking up." Under no circumstances will this bio-fascism be relinquished. None. No logic or data or facts matter here. This is an NGO-mediated cult, and cults are impervious to logic and data. Only organized revolt will stop them.
I wish I disagreed with you, but sadly I don't.
Great article, great opinion, thx! I notice now that the next straw the 'but it is really really bad!' convicted hold on to, is 'long covid', it is irresponsible to let people get ill at all, at any cost, because the long covid is so common...
Do you have an opinion on that?
First, I think the numbers for it are highly exaggerated.
Second, the 'syndrome' is partially psychosomatic: so much fear for the virus (most sneeze a bit for a few days), that to have the deadly virus is devastating; overlaps with ME, lyme and other (self diagnosed) hard to diagnose (and treat) similar conditions; UK post-vaccination indicates recovery of long-covid-ers (hard to explain physiologically), and some also do test negative.
i have seen literally zero evidence that long covid is any more common, significant, or dangerous than long flu or long pneumonia. any respiratory disease can cause lasting effects. but the definitions being used for "long covid" like "difficulty concentrating" or "low energy" overlap so much with depression that finding any meaningful number in a self reporting study is all but impossible.
you can see how clownish some of these claims are here:
https://boriquagato.substack.com/p/mark-it-covid/comments
The long-COVID brigade seems to have dispensed with the requirement to demonstrate a positive Covid test at any stage now. So presumably most reports are genuine symptoms but arising from prolonged fear and stress from pro-lockdown psychological manipulation and general fear propaganda. And maybe just wearing masks...
Indeed, the symptoms are real - even if psychosomatic - and need their own treatment, but as you infer, the cause needs to be clear to have a sound evaluation on what measures are appropriate and proportional. The long-covid-ers are genuine - from their perspective - but...? What happened to or is lacking from our scholing system - some critical thinking and statistics for everyone?
of interest, the google search prevalence for terms like "fibromyalgia" and "chronic fatigue syndrome" dropped sharply right when searched for "long covid" spiked. this is supportive of the idea that a subset of people with vague or generalized persistent symptoms simply jumped from one explanation to another.
Thx for quick response, missed that article from April 11, but is hard to keep up with the long reads by the Bad Cat... :)
sign up for the emails. it don't cost nuthin'.
el gato malo, very glad I found this link/e-mail thread!
Twitter is useless.
AAnyoe under 60 in good health should not vax.
Zeno paradox argues against the vaccine, ultimately only solitary confinement would be accepted.
The answer to long covid is its: low prevalence, short duration and image/accuracy of diagnosis.
That said prevalence of vaccine long term effects that look like long covid and worse would have Zeno accolades argue against vaccine.......
Vaccine after all causes immune response are similar to the infection! That is you could get all the effects as well as the autoimmune issues!
Also we have variants and the innuendo that corona virus is vastly mutating like flus, which is not implied by low prevalence in corona cold societies..
...as an aside, the vaccine hucksters have *already* announced the need for "booster" shots. Pfizer promised, yesterday I believe, that theirs would be ready by end of 2021. Ooh, that cash is already being counted!
The mRNA vax causes your body to create antibodies against the spike protein the mRNA causes your cells to put on their surfaces. Those antibodies are made by your immune system. What Pfizer is implying: your immune systems forgets, which is not seen in natural immunity that impacts your immune system in a similar manner.
I think we see a permanent vaccine "cold war" like the military industry complex profits from.
Actually, I misspoke. What Pfizer said was, they would have shots that would protect against the (apparently many) variants by end of the year. One could argue that is not a "booster shot" but, in fact, a message to a create antibodies to a different spike protein? That said, I agree with you, IFAIK, natural immunity takes such variants into account. I guess the jury is still out on if an mRNA "vaccine" does the same thing. Not that I believe in conspiracy theories, but it would be more profitable if either: the vaccines did not; or you could convince people that the vaccines did not!
Yes, perpetual pandemic is as good a business model as Lockheed's for the perpetual war threats. Good, solid profits when US buys 100's of billions and shields liability.
I don't agree with your view that "anyone under 60 in good health should not vax". I oppose mandated vaccination, but there's (at minimum) a significant part of that population for which I see a clearly positive cost-benefit.
I sat down last summer and worked out a range of quantification of COVID risk for my own demographic (healthy mid-40's). I had CDC reported COVID fatality data through that point in time (end of July), which included ~157k reported COVID deaths. To get around the denominator issue (actual number of infections), I used a range of assumed overall U.S. IFR's from 0.25% to 1.00%. (I'm aware of Ioannidas' estimate of 0.15% global IFR. The U.S. population is significantly older than the global average, so it's reasonable that U.S. IFR would differ from global.)
I also had CDC data that allowed me to look at reported COVID deaths and cases for ages 40-49 as either "with known underlying conditions" or not". (Important note: I am *not* at any point using a case fatality rate as a measure of risk. I use population-wide IFR's as the measure of fatality risk, but work with relative death / case #'s to try to determine relative risk if a person does or doesn't have an underlying condition.)
With these proportions - plus U.S. demographics by age group - one can adjust to get a view of fatality risk *if contracting COVID* (i.e., an IFR for an age range, with or without underlying conditions). My conclusion was that COVID IFR for a person who is healthy and mid-40's ranges between about 0.039% and 0.156%. At the lower number, that's 1 death per ~2,600 infections. That's fatality risk equivalent to ~3 years of U.S. population-wide risk of vehicle accident fatality. (The higher end of that IFR range is equivalent to ~12 years of vehicle accident fatality risk.)
There are of course bad outcomes - such as being hospitalized for several days, which is no fun - short of death. That can happen with either COVID or a traffic accident, so for simplicity I've assumed those are roughly equal.
(BTW, my conclusion at the time was that COVID was something about which to take some modest precautions, but that I shouldn't fundamentally change how I lived my life. That's for personal risk. Trying not to expose older individuals such as parents was an additional consideration beyond personal well-being, however.)
Now, that risk is of course conditional on getting enough exposure to SARS-CoV-2 to be infected. I would argue that's pretty much an inevitability if everyone under 60 takes Ed's advice and completely avoids vaccination. My assessment is that the risk of a severe outcome from the vaccine - meaning enough to require hospitalization, so not even fatality - is most likely at least a couple orders of magnitude lower (1 in hundreds of thousands). That risk isn't fully known even after clinical trials, but 100+ million people globally have now received the two mRNA vaccines (Pfizer/BioNTech and Moderna). If I could hypothetically get a similar vaccine that would make me essentially immune to traffic accident risk for the next 30,000 (or perhaps more) miles that I drive, I'd do so without hesitation.
I see a lot of the usual arguable points. I do not usually respond to gish gallops.
As of 19 Apr 2021, .09 of US has shown up as "cases" on worldometer. That is 9% prevalence in 14 months, since last June massive numbers (405M) non random testing of mostly asymptomatic subjects.
Risk is plotted P of consequences vs deleterious effects of consequences. P on X axis consequence on the Y.
My observation is under 60 healthy take the 9% chance of the infection rather than 99% (in risk 100% is a casualty not a risk) chance of effects of foreign DNA/mRNA wandering around your cells, induced protein synthesis, and B/T cell effects that last forever.
My personal risk chart said nah! I am over 70 and healthy, I took the vaccine in the AZN trail bc they needed older subjects, science!
I do not have as long to live with my choice as a 60 yo!
"Cases" are known to understate actual infections, though nobody is sure of the exact magntude). Actual cumulative prevalence has been more than 9% in 14 months.
That's why case fatality rate (CFR) is a basically useless stat. That's why there's been so much debate about actual IFR's: nobody *knows* the correct denominator.
Ionnaidis (and others) estimate IFR by trying to find estimates of true infection numbers. Typically those are serology surveys that sample populations for antibodies in order to estimate true infections. (Perhaps those are adjusted for sampling bias, or used as guides to extrapolate more generally about the relationship between actual infections, case counts, and test positivity.)
And here's the key - if estimate of cumulative prevalence to date drops, then implied IFR increases. Assumed U.S. population-wide IFR's of 0.25% to 1% imply ~50 million to ~200 million actual infections, not the ~30 million number Ed's citing (cases).
In other words, if only 9% of the U.S. population has actually been infected to date - which is wildly unlikely, nobody looking at testing details thinks that tests have identified anything like ~100% of actual infections - then you don't want to get it as a healthy mid-40's person because you'd have about 1 in 400 chance of dying if you did.
Thanks,
Another piece of the calculation (which I don't know how to estimate) is that the population that has made it thus far (~ 1 year) without getting sick is presumably less at-risk than average.
I too miss the Bad Cat on "the Twitter" but am damned glad to run into his feline musings here.
At this point, the early treatment discussions are another big tell for me that COVID public health is about totalitarian control and nothing else. You mentioned budesonide, do you have an opinion about ivermectin? It too seems effective but there's a massive noise machine against the signal.
The two biggest risk factors that I can find (after age, which you can do nothing about), are obesity and vitamin D deficiency. How much better off would we have been if government had "mandated" an hour-long walk in the sunshine on days it was possible?
Of course, that wouldn't have the side effects of swinging an election or trillions of printed dollars raining down on the well-connected.
Exactly. The mandated reactions, by and large, had the opposite effect from helping. See: cancelation of outdoor athletic events in NY, last summer!
Great post, keep it up. Miss you on Twitter, but little blue bird will be gone soon enough.
Thank you for these posts. I have come to rely on you for clear thinking and accurate information. I look forward to your posts every day.
The Cleveland Clinic COVID-19 hospitalization calculator https://riskcalc.org/COVID19Hospitalization/ shows a 3.5% hospitalization risk for a 62 yo white male at an obese 30 BMI and a double 7.2% risk at a thin 20 BMI. They are saying being obese is much better! Follow the science!
Fact-checkers didn't exist until the truth started getting out....
I LOVE you analysis have since the start!! Have you seen this article? More stats from the other more lethal pandemics.
https://coronanews123.wordpress.com/2020/05/25/equivalent-of-150000-died-in-u-s-in-1968-and-1957-flu-epidemics-no-closings-no-masks-no-distancing-woodstock-not-canceled/
you get into too many comparrison instead of making 1 strong one. i preffer the car + shower. and pump up the numbers to 95% .. even with that type of prevention people WILL NOT TAKE the measures
PS. why is the swiss chese image in the thumbnail but not in the article?
i feel like you are too wordy, your points lose their punch with too many words and not simplifying enough.
take "cliff notes: you have about a 0.9% lifetime chance of dying in a car crash in the US. your risk of getting covid post vaccination and then dying from it is on the order of 0.015% even if we add no other mitigations and assume you have a 100% chance of getting covid without a vaccine. this is 1/78th the risk of death by car crash over a lifetime."
vs "cliff notes: you have about a 0.9% lifetime chance of dying in a car crash in the US. assume you have a 100% chance of getting covid without a vaccine. this is 1/78th the risk of death by car crash over a lifetime.
I think this is your best post yet. Keep it up!
freshman in college in Fall 1968. no memories but we had Vietnam every evening on the 30 minutes national news. LBJ ran on no mushroom clouds in the background. Public health propaganda was not needed in the 1968 election. Not that I made time to see Huntley/Brinkley!
As a 70 year old with low BMI, regular exercise, low blood sugar and on Vit d for years I took the vaccine, largely because I live with a 72 yo who hates Trump! And thinks .00007 risk is too high!
Absolutely fantastic post. My fear is the inability or, in some cases, unwillingness of the populace to appropriately gauge risk will only further embolden health and government officials to continue this safety theatre charade indefinitely.
In any event, thank you for these posts. It is comforting to know critical thinking isn’t completely dead.
The shorthand way of looking at what’s been imposed in the name of covid protection is, Would you shoot yourself or your children in the head (or abdomen or leg) to reduce the chance of dying from another gunshot or some other everyday event?