



pfizer says their covid vaccine works in kids 5 to 11. does it?
comparing the possible benefit and the likely risks

pfizer came out this morning with the aggressive claim that their vaccine “works in kids 5-11 years old” and that they will soon seek approval.

this is clearly a cash cow for them and parents and school boards beset by carefully inculcated night terrors about the risk covid poses to their children and to schools are all desperate for “a solution” that feels like “doing something.”
this creates a strong incentive for pfizer to seek to overstate benefit and for scared parents to want to believe them.
but we need real answers.
because medicine is everywhere and always a risk/benefit decision.
there is a reason that you do not take fentanyl to cure a hangover (despite the fact that it would).
that reason is not that you are “anti-medicine.”
so let’s put aside all the moralizing and grandstanding and just look at the data. performing risk/benefit calculations is being PRO vaccines, not a dogmatic antivaxx position.
it’s a simple equation:
is BASELINE RISK x RISK MITIGATION > RISK FROM MITIGATION
that’s the whole question, always was, and always must be. so let’s fill it in:
baseline risk:
firstly, the risk to children aged 5-11 from covid in absolutely minuscule. it’s very rare for them to get anything past a mild case that passes quickly and those that do are almost always children with serious comorbidities and risk factors.
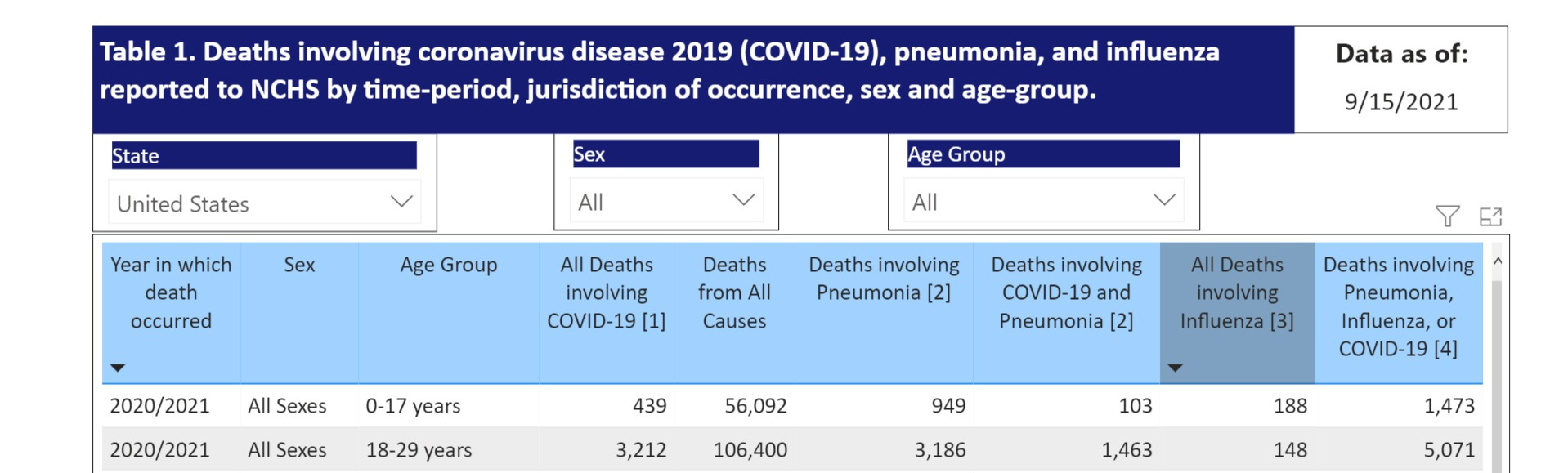
in 19 months, there have been 439 pediatric deaths from covid in the US. this is 72% lower than the number who have drowned in the same timeframe (and less than half of pneumonia). it annualizes to a 277/year rate.
this is a annualized population fatality rate of 0.000003105. (73.1mm kids)
0.00031%.
1 in 322,061.
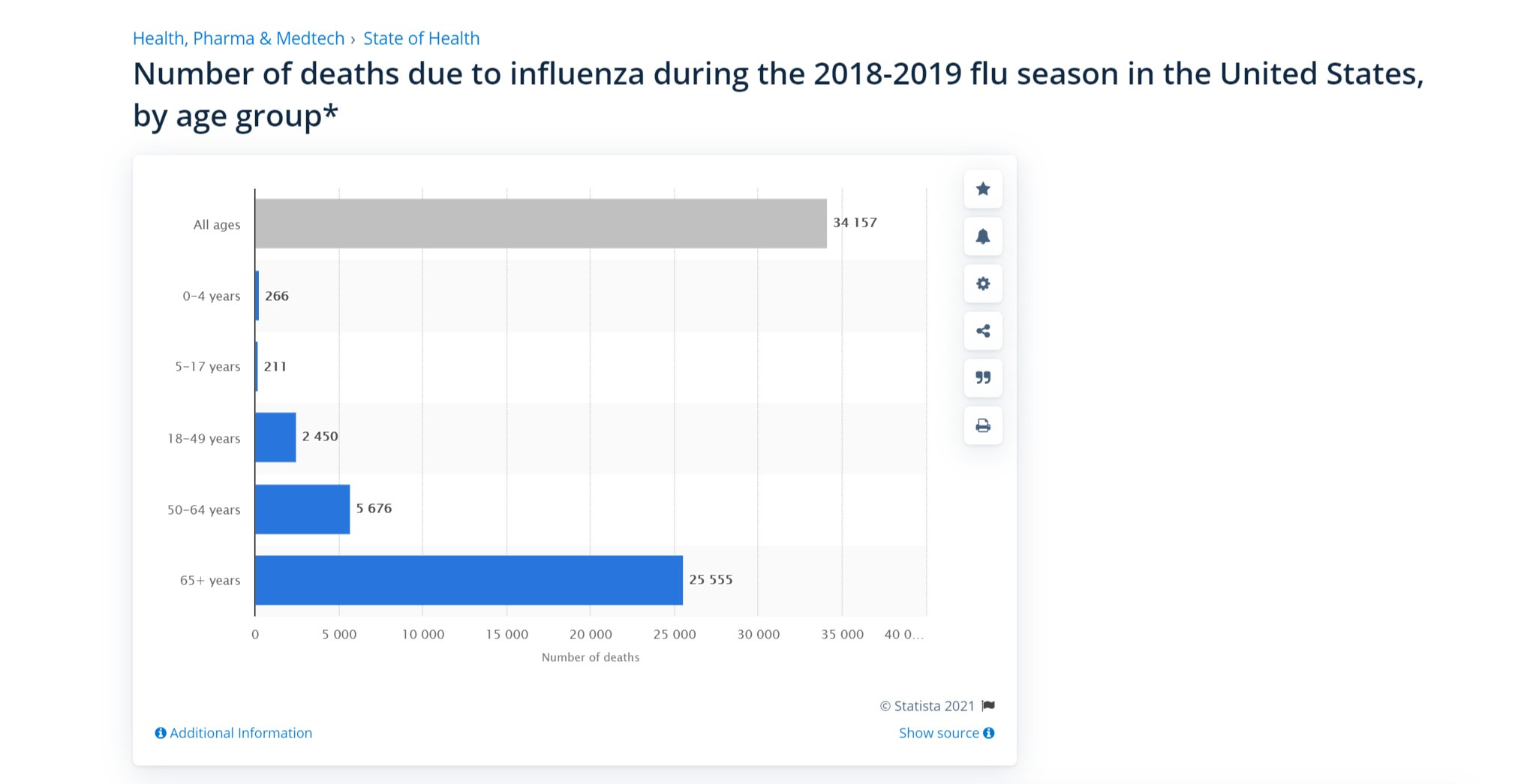
note that this is lower even than (the incredibly rare) flu deaths count in this demographic.
467 in one flu year means 1 in 156,531. it’s basically 2X as deadly to this group as covid.
and we’ve certainly lived with flu for a LONG time. kids have lived with it, schools have lived with it, and really, no one was terribly worried.
if you felt sick, you stayed home. wash your hands. cover your mouth when you sneeze or cough. that was the response to a killer of children twice as deadly as covid.
so let’s keep that in perspective.
and no, hospitalizations were not “off the charts” either.
this covers about 10% of US population, so let’s multiply it by 10.

39,840 in the whole of the pandemic. 0.00054.
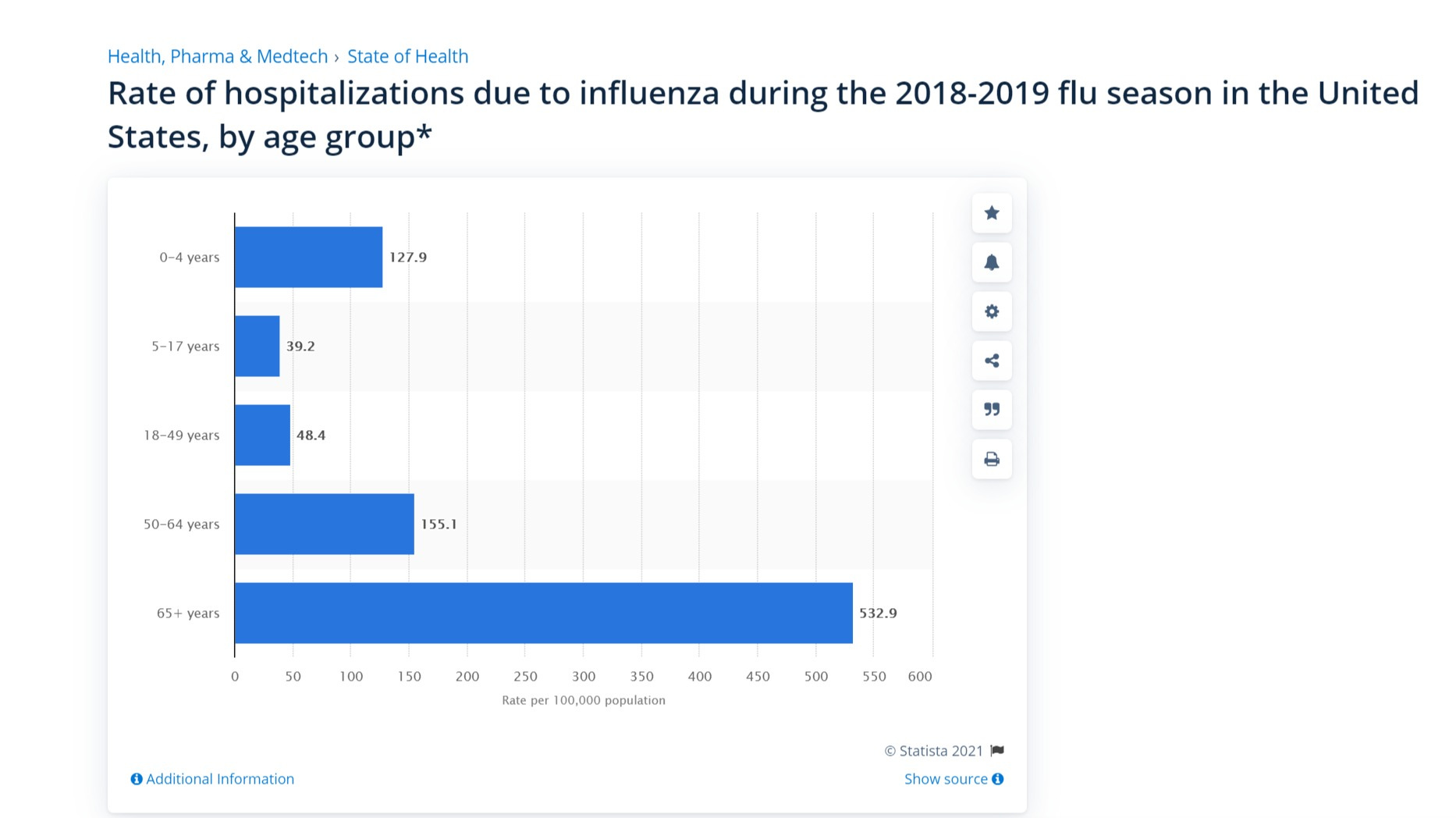
this annualizes to 25,160. 1 in 2905. this is 34 per 100k per year.
compare that to flu:
it’s the same rate for 5-17’s and 1/4th the rate for 0-5.
covid is not more dangerous to kids than flu, it’s less so, and no, “long covid” is not some aggressive new thing. it’s no more common than lasting effects from other respiratory illnesses and in many studies, could not be statistically discerned from control group in kids that did not even have covid. 53% of control reported “symptoms.” hardly surprising given the generality of the symptoms and the stress kids are under.
so look, we have a REALLY tough bar here to prove risk reward.
there is just not that much baseline risk to even mitigate.
even if pfizer vaccine is 100% effective for this cohort, they have a maximum benefit per child year of:
1 in 322,061 for death (0.31 per 100k)
1 in 2905 for hospitalization (34 per 100k)
it is unlikely to stop cases. it has not in any other age groups. these vaccines appear to be completely non-sterilizing and may be making spread worse especially during the 2 week period of negative vaccine efficacy post administration. (that seems to be being deliberately misallocated to the great benefit of reported vaccine efficacy)
risk mitigation:
so how well will this vaccine reduce risk in kids? the answer seems to be “we have little idea nor any clinical outcomes data whatsoever.”
the data pfizer is currently presenting is all biomarker data. there is nothing in it showing any sort of clinical outcomes. this is, to put it mildly, a very aggressive and possibly dishonest approach.
they did not prevent any “cases” or “deaths” or “hospitalizations.” this was too small a study and the kids in it got sick at far too low a rate (as predicted above) to be relevant.

this is not study data, it’s the data you’d use to validate DOING a study. even pfizer’s more aggressive boosters (sorry, irresistible) had somewhat qualified praise.
and others were less sanguine:

what are the risks of taking the vaccine?
this was a reduced dose of vaccine. it was about 1/3 the adult dose and this makes sense given the likely weights of those taking it. (honestly, this should probably be weight administered overall.)
they did not provide actual data, but according to the pfizer press release it resulted in:

and this is useful as that is data that we already have. in fact, i looked at it once before and found some significant issues on risk reward for 16-25.
we can pull data from the CDC here.

keep in mind that this data is cumulative. you need to take 2 doses to be “vaccinated” so you need to cross both hurdles.
so, in the 16-25 they suggest as comparable, we see:
21.9% unable to work. (21,900 per 100K)
35.5% unable to do daily activities. (35,500 per 100k)
1.3% required medical care. (1300 per 100k)
0.3% required ER or hospital stay. (300 per 100k)
these are massive, quite literally unprecedented numbers for a modern vaccine. this data from the FDA public session during friday’s panel meeting really dives this home

note that VAERS reporting is really just a “tripwire” to show that a signal exists. it is certainly meaningfully incomplete and is certainly underreporting bad outcomes.
whether the real number is 3X or 10X this number is a matter of debate but it’s certainly consider higher than this data. 386 million doses of vaccine have been administered in the US (181 fully vaxxed). if the ratios above from CDC hold, that would predict 17.26% being “unable to do normal daily activities” (blended avg) and thus 66.61 million VAERS reports. there are 521k. that could imply undercounting on the order of 128X for symptoms. (this may not be as crazy as it sounds. i know A LOT of people who got quite sick from vaxx, esp post dose 2. pretty much none reported to VAERS. but, that said, i am not at all confident in this admittedly rube goldberg methodology, esp if it would hold for deaths, and if others have a better idea on how to do this, please share.)
so let’s sum up:
to avoid criticisms of “cherry picking” i am going to steel-man the vaccine case.
i will presume, despite no clinical evidence, that vaccines are 100% effective in 5-11 year olds and need only one annual booster.
i will also presume that the VAERS count of adverse events is complete and captured all relevant data. thus 7,662 deaths from 211 million people with at least one dose of vaccines = 0.0000363 = 3.63 per 100k
i will assume that ALL US kids will get covid and than NONE have pre-existing immunity from having had covid and recovered.
then, we can assess this:
is BASELINE RISK x RISK MITIGATION > RISK FROM MITIGATION
and because we’re assuming 100% risk mitigation, that term becomes 1.00 and thus the equation collapses to:
is BASELINE RISK > RISK FROM MITIGATION
this is the best possible case for vaccines in this age group. but like the older kids before it and even healthy adults overall, it does not look positive.
in fact, it looks TERRIBLE
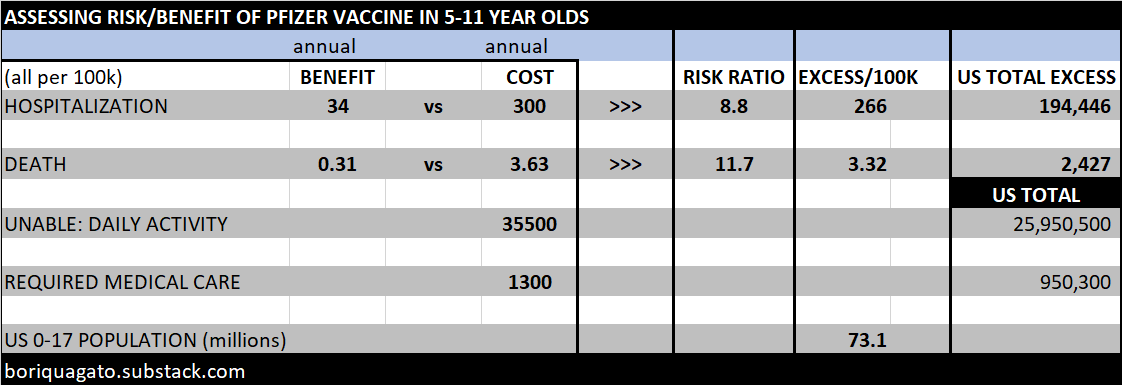
the cost of saving 34 hospitalizations is 300 hospitalizations. 8.8X risk to reward.
the cost of saving 0.31 deaths is 3.63 deaths. 11.7X risk to reward.
thus, even assuming NO prior covid exposure or acquired immunity, vaccinating all of america’s children's from 0-17 would result in:
194,446 dditional hospitalizations (4.9X those in all of covid so far)
2,427 additional deaths (5.5X those in all of covid so far)
vs literally letting every single child in america contract covid.
it would pile on 26 million kids unable to perform daily activity because they were too ill from vaccine reaction. (vs a disease that’s mostly mild or asymptomatic for them)
it would add nearly a million additional kids requiring medical care.
(i lack good figures to comp these last two effects to, but if someone has them, i’d love to see them and if someone wants to claim “disease is worse” i’m going to need to see good validation of that claim esp as vaxxed means everyone and disease is always less than 100% prevalent and probably half the kids in the US have already had covid.)
even as a best case, this mitigation looks simply unsupportable for kids.
in a real case, kids probably face 1/2 or less this risk from covid due to naturally acquired herd immunity and risks (esp death) could easily be 10X or more what was estimated here.
for under 17’s the risks are so wildly out of line that even if i’m off by a factor of 10 on risk reward (unlikely as it almost certainly goes the other way and i understated risk and overstated reward) this is still a bad idea. the safety margin on this data claim looks wide.
one of the reasons so many of us (me included) trust vaccines like MMR so much is that they are incredibly safe and effective. they had decades of testing before going into widespread use, they treated truly dangerous diseases, and they did more than just mitigate severity. they stopped spread.
the pfizer vaccine does not. (none of the approved/EUA vaccines seem to) and they pose very high risk for, especially in kids, near zero reward because baseline risk is so low. it’s a fraction of the flu risk no one panicked over for 100 years.
this sort of societal mitigation strategy is all about the odds. you need to understand the real risk, the real rewards, and make the choice that’s right for you.
do you own work. double and triple check mine. invest in knowledge about your own health options, it’s an investment that pays off. bigly.
and it’s worth remembering that not all the people telling you the odds are actually on your side.
make your own determination about when the odds are in your favor…










So, just to get this straight…..
1. Less than 1500 5-11 yo’s receiving an mRNA vaccine for the first time qualifies as a “safety” and efficacy study.
2. An 11 yo requires 1/3 the dose of an EUA therapeutic as a 12 year old.
3. We no longer need to use clinical endpoints in studies because the desired impact can’t be proven, and instead substitute lab titers as a proxy for a drug’s clinical effectiveness.
While I love data and analysis, and even data analysis, I figure we can likely come to one conclusion now and use it going forward: Rule One: Pfizer is Pfull of Shit. Rule Two: When in doubt, or when presented with *any* additional data or narrative, refer to Rule One.