



RSV vaccines in pregnant women and infants
same companies, same questionable practices and sales pitches

it certainly seems sensible that societies should evidence strong concern over the welfare and safety of pregnant women and infants. after all, societies that do not have a tendency not to be societies anymore in pretty short order.
but this is an impulse around which one must be careful because as is always the case, the precautionary principle cuts both ways and often warns against itself.
are you advising pregnant moms to stop smoking and not take PCP and urging them to eat well and get plenty of sleep or are you engaging in bloodletting for maternal fluxes and prescribing thalidomide for morning sickness?
the really obvious ones tend to be easy to spot (at least after the fact) but many are far more subtle and take some real analysis done openly and honestly to make sure we’re engaging in good care and not the predatory profiteering that is the flip side of concern and takes it too far into “taking advantage of the worried.”
and this is what has made me so concerned about the fast and loose manner with which this game has been being played so frequently of late.
“hide the ball to sell more drugs” is not something one ought to tolerate when speaking of medicine. i am not anti vaccine, but i am anti negative net utility pharma products sold with misleading research.
and i fear they are at it again.
those of discerning cattitudes will be familiar with this refrain.
it is the basic ground truth of the medical profession and all that attaches to it.
it is not “anti-science” to say so. it’s anti-reason not to.
so here we go again.
pfizer is once more seeking to push a vaccine upon the gestating, this time for RSV.
and many of the same folks are out proclaiming “safe and effective” based on THIS STUDY published in the NEJM.

but is it?
“babies most at risk” sounds scary, but it’s a basically meaningless term as a form of risk assessment until we know a great deal more about that risk so we can compare it to other risks (like taking a drug). and it seems this study and its professed conclusions are going to great lengths to avoid making such comparisons easy. i suspect this is because:
this study failed to reach statistical significance on some important endpoints
efficacy was considerably lower on disease overall (and not stat sig)
using relative vs absolute risk reduction when discussing vaccines inappropriate for risk/reward calculation
safety not as advertised
risk reward is negative
and the study design itself was rigged using a trick to make “placebo” look worse
let’s take a look:
1.
right in the abstract, this study tells us it failed to reach statistical significance for “medically attended RSV-associated lower respiratory tract illness” over a 90 day period. it IS however claiming efficacy for “severe” LRTI over the same period. stop me if you’ve heard that one before.
right there it makes me wonder why viki is pushing it as "effective" as this study was a clear fail on generating any sort of sterilizing immunity and we’ve seen all manner of the sorts of problems that non-sterilizing vaccines produce around OAS/antigenic fixation.
oddly, its authors are claiming "effective" despite this.

efficacy also seems to fade over time.
this seems like another statistics game with high risk downstream outcomes around herd antigenic fixation that is unlikely to have any meaningful effect. vaccines are not magic, they simply train your immune system to resist further incursions by a pathogen. but they have no track record of working for viruses that are not “one and done” (like measles or chickenpox) where your body can generate durable immunity from one exposure.
remind you of anything?
2.
relative efficacy for "medically attended RSV associated lower respiratory illness was considerably lower for vaccine. (57% vs 82% claimed for severe)
the error bars reach down to 14.7%.
again, looking very leaky and like it fades.
this was not stat sig and it’s clearly non-sterilizing.

3.
now the doozie: claimed efficacy is relative risk reduction, but does not speak to absolute.
this is extremely misleading when used in a vaccine that will be given the healthy people.
imagine buying insurance. 50% drop in a 1% risk is very different from 50% drop in 50% risk. you’d pay very different prices for that coverage. medicine is the same.
absolute risk/reward matters and “relative risk reduction” is an entirely inappropriate way to gauge a vaccine that will be administered to healthy people.
this is 100% done on purpose to make the numbers sound big and to make assessment of risk ratios impossible and trust me on this one, companies like pfizer do not make basic science mistakes like this. they make choices.
usefully, absolute risk reduction is already in the charts in the study, it's just not being foregrounded.
0.9% of infants had severe in placebo vs 0.2% in vaxx
so taking this at face value:
7 infants per 1000 born to vaxxed moms would avoid severe
9 infants per 1000 born to vaxxed moms would avoid going to the doc
that's the purported benefit of this product. (red mine)

note that “medically attended LRTI sounds scary, but mostly isn’t.
it’s “you took your kid to the doctor for a cough or a runny nose.” it’s a pretty pedestrian outcome.
4.
but now we need to look at risks.
the study authors blithely claim "no safety signal was observed" but this looks like a very iffy and dismissive claim hiding behind the very stat sig they failed to reach on sterilizing efficacy, and let’s face it, claims of “safe” have been made a bit carelessly of late.
so let's look at adverse events (AE’s), because this is not good. (red mine)

5.
i'm going to build a spreadsheet to make this easy to see:
the categories are different and so is the timing (3 months on benefit, 1 month on adverse events which slants comparison in vaccine favor) and so they have made it hard to compare, but it doesn't matter.
the signal is stark.
risk reward here looks awful.

how one can look at this and say "safe and effective" is simply beyond me.
sure, we can argue error bars and stat sig on adverse events, but keep in mind, the study missed this on sterilizing efficacy too.
so you really need to pick a side of the street on that one and live on it.
it's no fair claiming "no risk signal" on bad outcomes because "error bars" while claiming "effective" despite "results did not meet the statistical success criterion” for “kept you from going to the doc.”
when we presume validity and adopt a unified structure of absolute risk reward: (ignoring the mild cases and mild AE’s)
every 7 cases severe RSV prevented in infants cause:
7 severe adverse events in infants,
4 more severe AE’s in moms,
and 2 life threatening mom results
along with 9 premature births
and 6 low birth weights.
it's just awful cost/benefit.
this is the kind of analysis those who would give a purportedly prophylactic drug to healthy people ought to be doing.
it's simple stuff and straightforward and the medical community knows this.
those ignoring it smack of agenda over rigor and sales over science.
simple heuristic:
when you see vaccines sold on "relative risk reduction" without reference to absolute benefit and risk, get skeptical.
it's not the correct way to do meaningful risk/reward assessment.
chances are excellent you're being sold a bill of goods.

6.
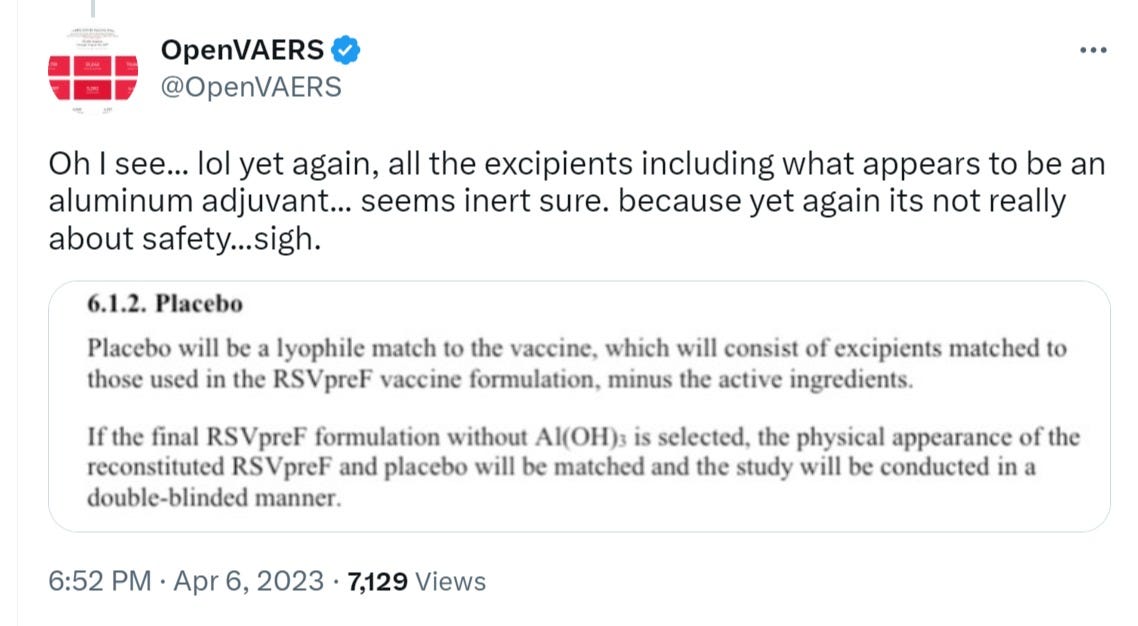
open VAERS (who has done so much great work here) had a great find that i had initially missed, and this is a SERIOUS confounder.
“placebo” was not placebo (like saline) it was something more noxious (aluminum hydroxide) used to mimic the appearance of the vaccine.
Health Hazards
Prolonged exposure to Aluminum (III) hydroxide it causes irritation in eyes, respiratory system, and skin. When comes in contact with water it causes a violent explosion.
now, we can argue about whether and to what extent being injected with such an excipient (bulking agent or stabilizer) causes harm (it’s also used in antacids etc), but 2 things seem certain:
it’s not going to be a benefit
those who chose “not to vaccinate” would not have been exposed to it
so, the “control” group is not really a control group. they are a group that almost certainly has elevated risk and likelihood of ill effect from the introduction of aluminum oxide to their systems.
this is an increasingly common (and seriously shabby) trick used in drug trials to make baseline adverse events look higher than they are to make drug look better in comparison. keep in mind we’re playing for 10th’s of a percent in absolute effect here. it does not take much to slant the scales.
when speaking of “interventions in healthy people” there is no justification for it.
it’s trial rigging and should be proscribed.
addendum:
here's another suspicious issue: overall medically attended lower RTI was essentially identical between the 2 groups.
RSVpreF vaccination did not prevent medically attended lower respiratory tract illness from any cause within 90 days after birth (vaccine efficacy, 7.0%; 99.17% CI, −22.3 to 29.3) (Table S8).
relative VE confidence interval -22.3% to 29.3% so that’s about as close to “cannot be distinguished from zero” as you’re going to see.
if it worked so well on RSV, why is there no risk reduction for infections overall? this is a worrying hint toward classification games or some form of other immune suppression akin to “stops covid, does not reduce all cause deaths” and we all know how THAT one played out… (or, it just means that RSV is such a tiny part of the LRTI universe that you’re playing for peanuts here) neither seems a strong case for a drug.
so, in the end there is just no case for this product in pregnant women.
it’s primed for failure as non-sterilizing, had low absolute effect on a low risk disease, and posed risks multiples of those purportedly mitigated even when using a rigged study design to make baseline risk rates look elevated above untreated population.
and while i am not an MD and everyone should make their own medical choices based upon their own situation, preferences, and advice from trusted advisors, i do know quite a lot of drug trial design and outcomes measurement and this is not a set of data i find in any way compelling.
it looks like significant net expected harm.











As I have posted on several sites already, we were thaught that pregnant women and lactating women do NOT take any drugs at all, Nothing. No aspirin, no benadryl, nothing at all. Certainly barely tested injections of chemicals known to be hazardous, should be totally out of the question. Any doctor telling a pregnant woman to take drugs or injections should loose their licence. This was known 50 years ago and it still stands.
I’m sure the relentless TV ad campaign will admonish pregnant women to get the RSV vaccine to show they care about their unborn child.