



relative excess deaths in the most "vaccine hesitant" minorities in UK
digging into more predicative data on overall survival rates.

whether or not covid vaccines provide overall mortality benefit has been a contentious issue since the beginning. infamously, they did not do so in their own vaccine trials. some have argued that this is because those in the trials were so young and healthy and so there was just not sufficient signal. (this, of course, can also be inverted into a criticism of using the vaccines in the young and healthy as well.)
the UK provides something of an interesting natural experiment to assess this as we have one population subgroup that has been extremely uninterested in getting jabbed.
black people in UK have expressed only 28%willingness to vaxx vs 84% in white.
i chose these two groupings because they map cleanly to the all cause mortality data. “asian” gets tricky as pakistani/bangledeshi differ quite a lot and are not broken out in the all cause deaths figures.

vaxx uptake data here.
in comparing these two communities, we immediately run into some challenges, foremost that the black community saw a MUCH higher death toll than the white during covid. i suspect this is due to a variety of factors including higher rates of obesity, heart disease, hypertension, and diabetes known to be severe exacerbating factors for risk of covid death as well as ethnic variances in ACE receptor expression. these all favor higher death the black community.
i used the UK excess death data HERE to graph this. the large divergence can be readily seen. interestingly, however, this variance was much larger pre-vaccination. campaign. i have marked the point at which vaccination reached 5% (and then rose steeply) in the UK on the graph.
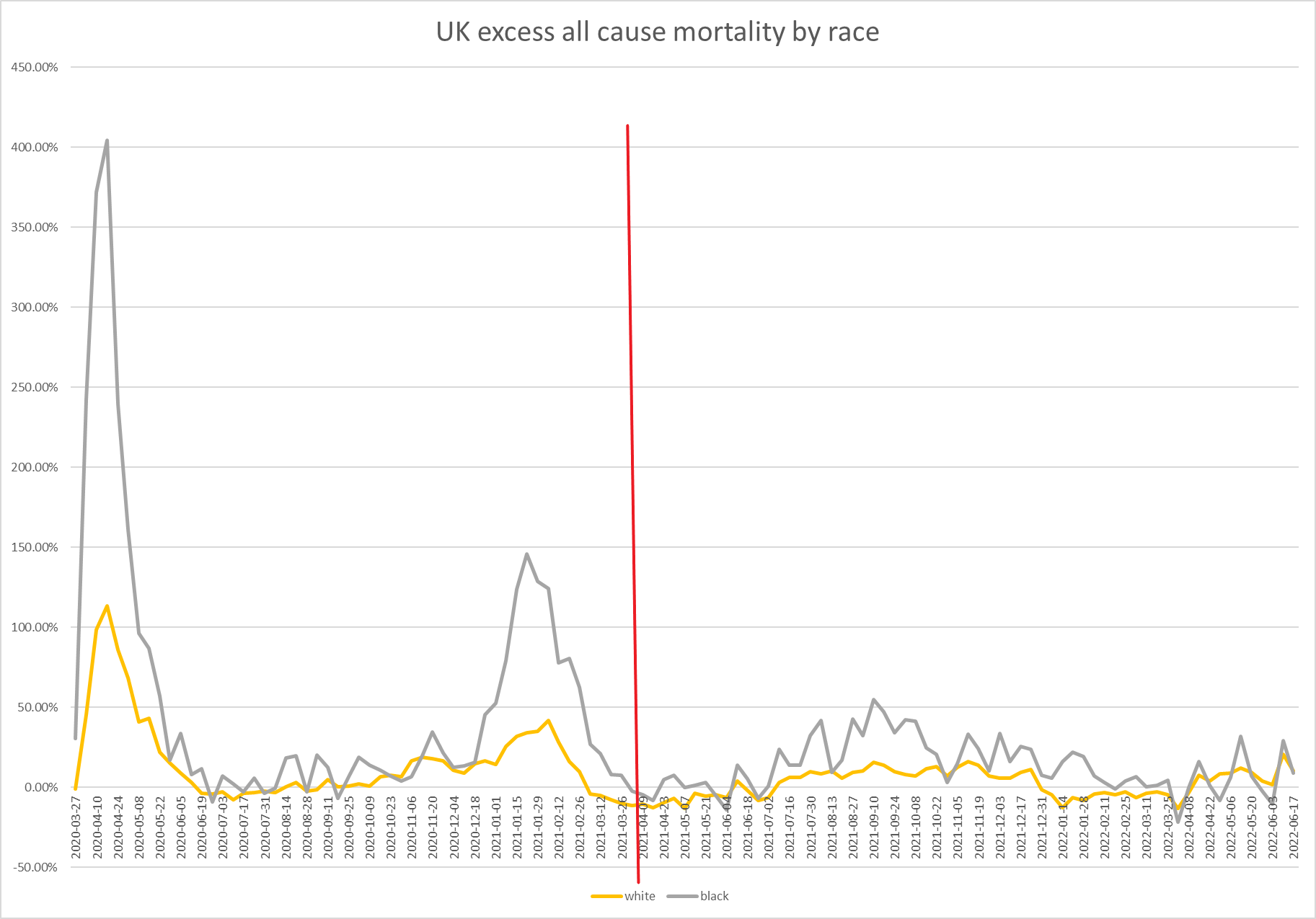
several things emerge from this immediately.
all cause mortality was much higher in blacks than whites during covid and remained so until ~april of 2022
around april 2022, this changed and the two moved into near lockstep
both dropped a great deal. this is consistent with less deadly variants and with cohort depletion
but the black cohort has seen more attenuation in excess deaths, especially recently. the question then becomes, why?
this is easier to see if we zoom in. this is only the period since vaccination began.
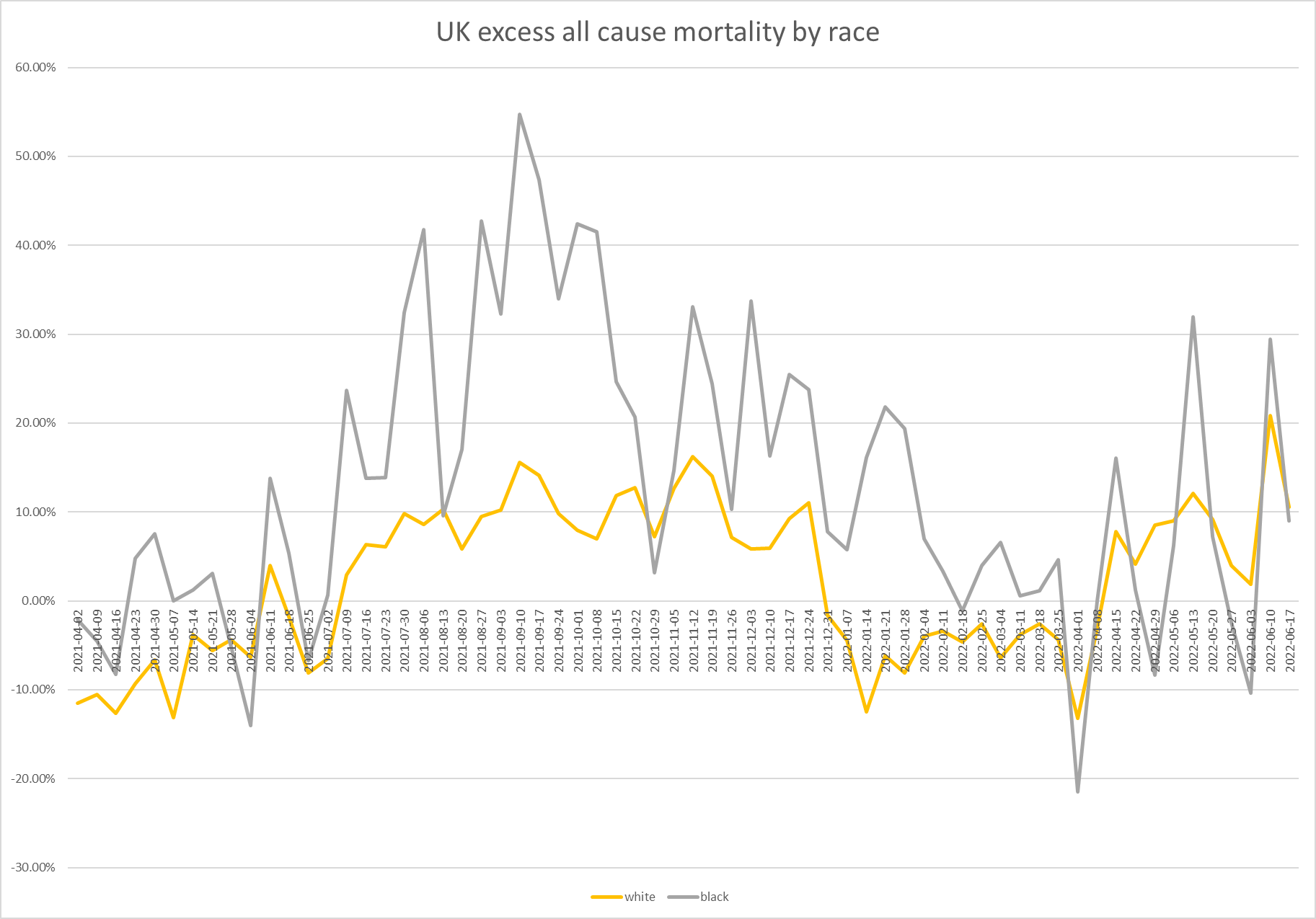
here we see something interesting. in the surge during sept-oct of 2021, black excess mortality rise exceeded white.
this would be consistent with vaccines working and generating overall all cause mortality benefit (or just racial variance). this aligns with what looked to be meaningfully positive covid death benefit (though not necessarily in all cause deaths) from vaccines seen in the UK around that time and with prior data on comorbidities.
but now look at the surge from april 2022 until present.
this apparent efficacy is gone. the two are now the same (despite the longstanding higher risk in the black cohort due to co-morbidity/disposition/etc)
two theories jump to my mind to explain this. the first is “dry tinder.” if the black community has had greater overall excess death then it has more intensely depleted its vulnerable groups. this should lead to less death going forward.
they certainly saw more deaths overall. here is cumulative excess deaths.
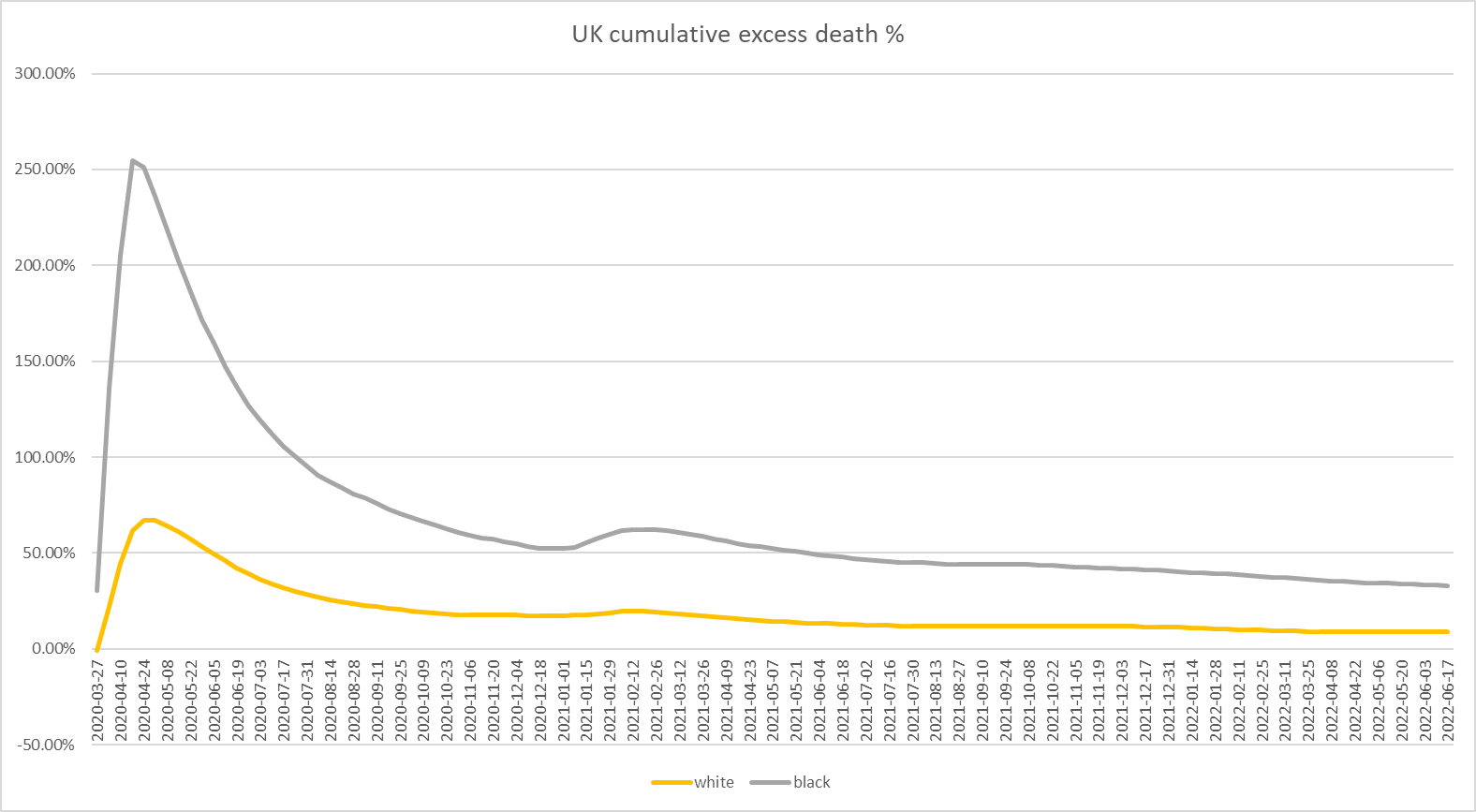
and here is the zoom in to just the post vaxx era:
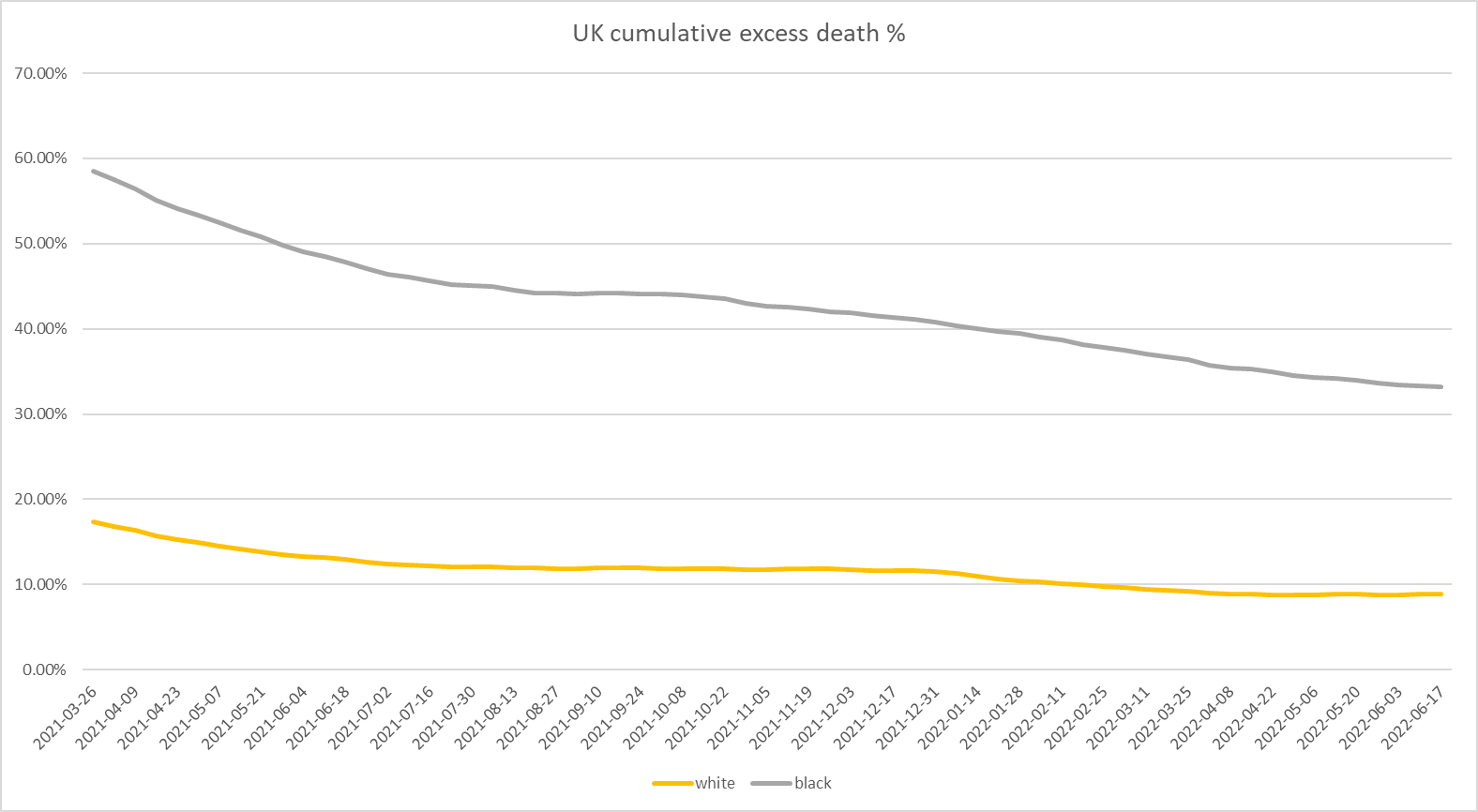
so, this driver may be having some effect. it’s certainly plausible. but i see some issues with this theory as well.
if you go back and look at the excess mortality by week charts above, this change was quite abrupt. if it were cohort depletion, you’d expect convergence in series to be more gradual. but it’s not. we really see no such signal until it suddenly emerges in the spring of 2022, specifically in april.
and i suspect this may be important because something else was happening in april too:
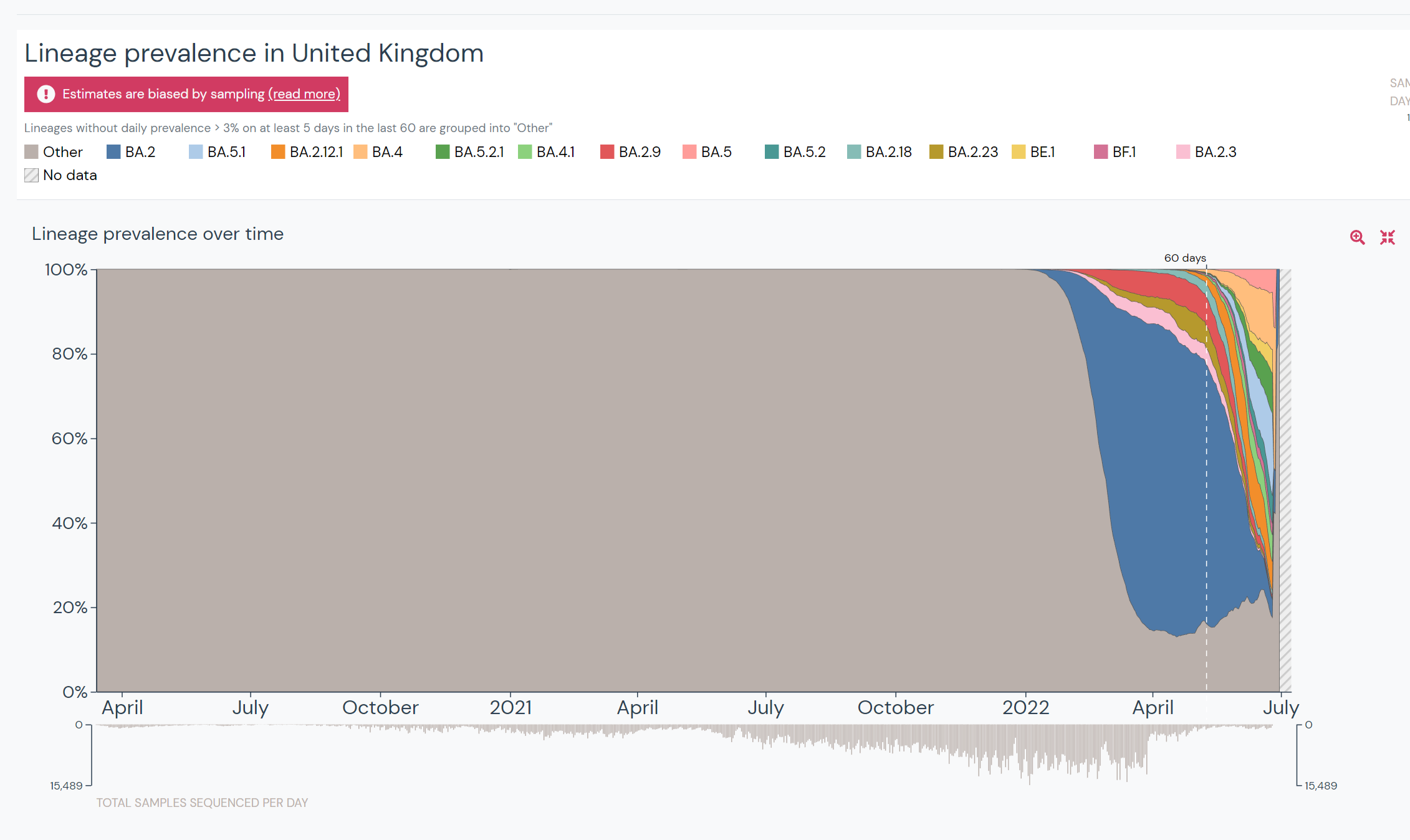
starting in march the BA.2 (and later) sub variants of omicron became dominant in the UK. and a few weeks later, the gap in excess deaths in the highly vaxxed white community and the low vaxx black community disappeared with great suddenness.
given the well established fears of the BA strains as “optimized vaccine escape/OAS variants that are actually vaccine enabled” this is more than a little provocative.
relative case counts in the vaxxed in the UK were exploding in the lead up to this same period. (more HERE)
alas, they then stopped reporting this and many other data series for vaxxed vs unvaxxed and the cynical side of me fears that the excess death shift may be giving us an indication as to why they did not want to talk about this any more especially as there is every reason to expect BA.4-5 to accelerate this variance further.
since the week ending 4/8, white excess deaths have exceeded black for an extended period the first time all covid at 7.8% vs 7.5%.
this was sudden and meaningful and seemed worth looking into.
as a sort of rough test, i set a baseline for each group based on their overall excess death from 3/27/20 until 3/26/21 when vax rates hit 5%. this gives us a sort of “unvaxxed” reference level.
(admittedly, there are a number of potential problems with this approach including not accounting for dry tinder and if people have some better ideas on how to get at this issue, i’d love to hear them)
i then compared current excess death vs baseline. the results were very interesting.
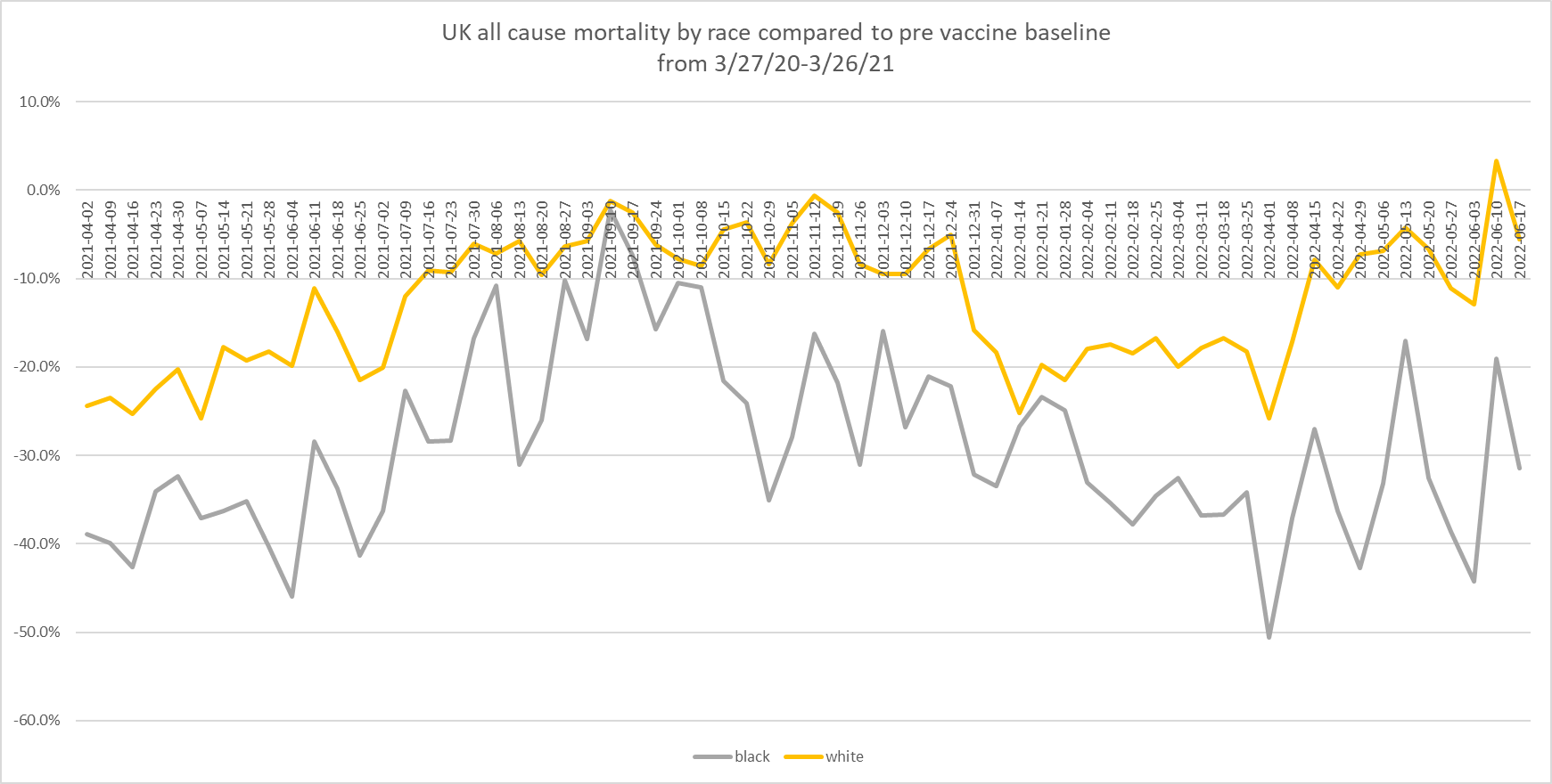
the greater levels of attenuation in the black cohort is readily visible. it’s largely flat to down since the beginning of 2022 and remains at about -30% vs baseline.
but the white cohort has been rising most of the year and rose sharply as BA.2+ hit. in june, some levels actually exceeded baseline.
this makes me increasingly suspect of “dry tinder” as an explanation. the prior lockstep in spread suddenly went away over about a 1 month period instead of gradually fading. that seems more consistent with a strong and temporally focused external driver.
to my eye, this seems most consistent with the following hypothesis:
vaccines provided some level of protection vs overall mortality that was equal to 0 or greater.
maybe they did nothing and whites just had fewer risk factors and/or got better care, maybe vaccines were providing some overall benefit, but this issue has now inverted.
high vaxx looks suddenly associated with higher risk and this looks to have offset a longstanding intrinsic variance.
if this is so, the next month or two ought to provide confirmation if this trend continues and/or relative excess mortality inverts further.
i actually suspect the that vaxxes were helping some on deaths and here’s why:
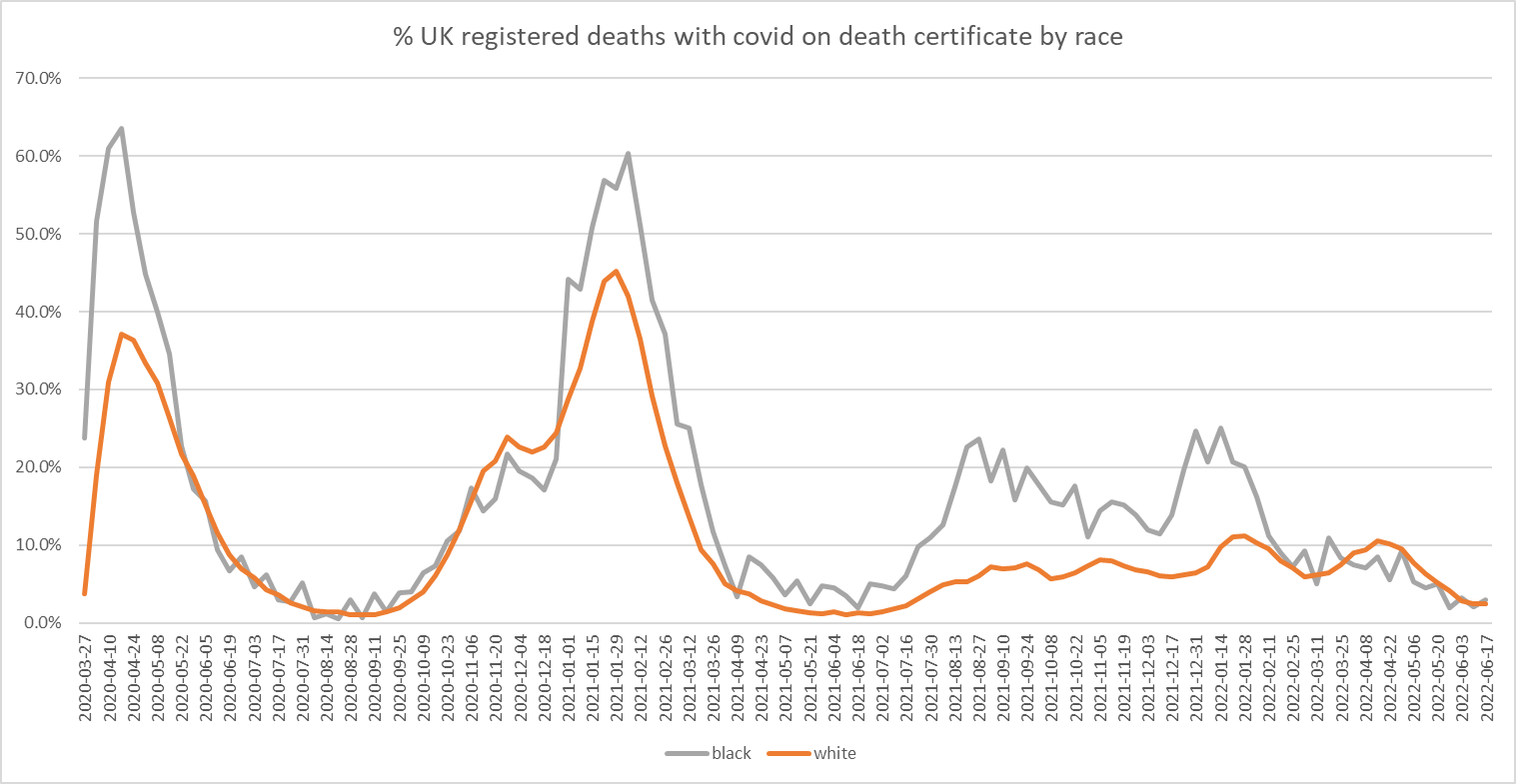
look at % of overall deaths with covid on the certificate.
it has been consistently higher in the black cohort.
but look what happened in april 2022.
it’s now become generally higher in whites.
that’s quite a switch on a relative basis.
note that this does not prove that VE is now negative for deaths in any given case. VE could still be quite high, say, 50%. but if you become 3X more likely to get covid, even 50% attenuation in deaths per case means a 50% rise on overall death experienced even if the vaccines themselves are causing no deaths (and they clearly are).
this is why these OAS and leaky vaccine driven viral evolution/herd antigenic fixation issues are so critical and why they should have ended these vaxx programs the second they realized the vaccines were non-sterilizing:
because if you push a leaky vaccine, especially one that elicits and fixates around such a narrow response vector, you end up in a spot like this.
you’ve created a lab that WILL create escape and vaccine advantaged variants. it is literally designed to. no other outcome is possible. then the BA strains show up and you start to see the effects and it starts to go faster and faster as the formerly recessive antigens become increasingly dominant.
that’s just evolution: always looking, testing, probing, trying to find a path for the water to flow downhill. selfish genes seek to replicate. give them new selection pressures, you select for different things. this is part of what makes omicron so interesting (and potentially telling). it was not a descendant of delta. the two have no common ancestor unless you go back to even before alpha.
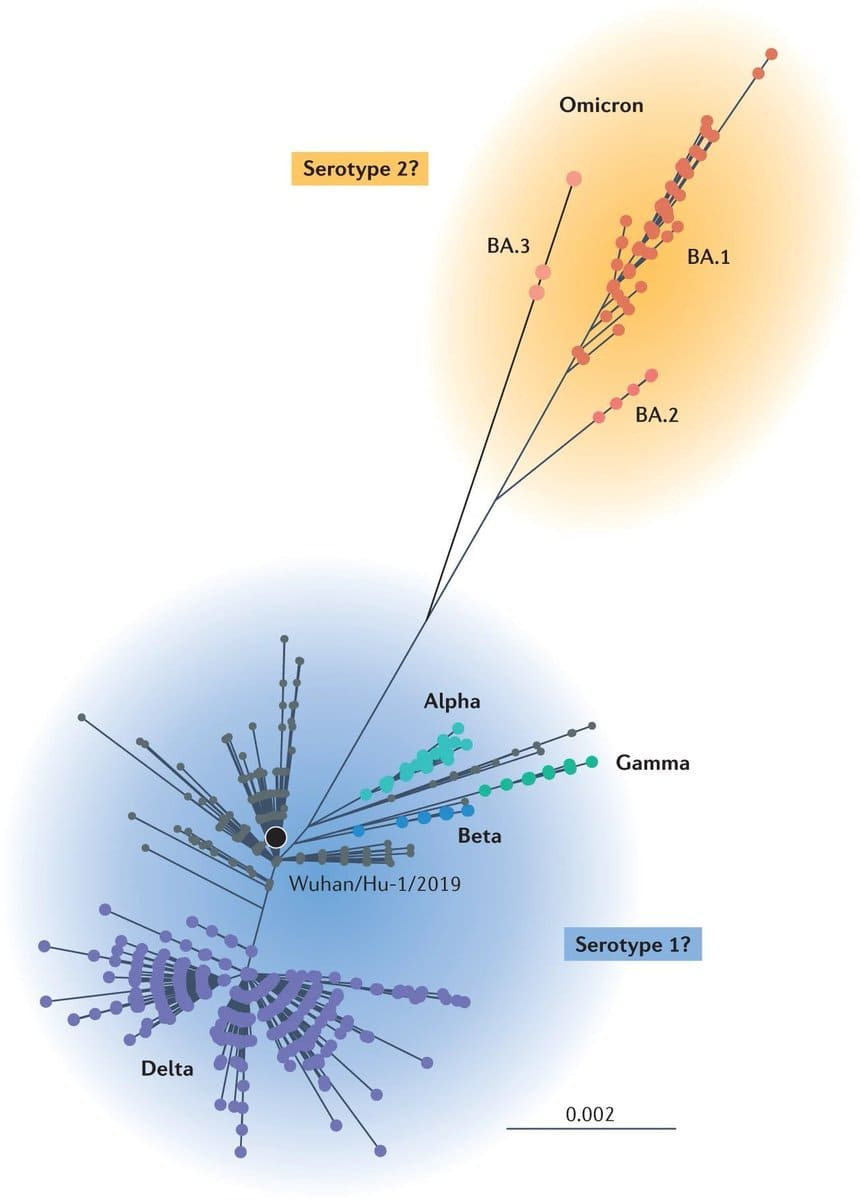
we’re into a whole new serotype and this occurred as a major throwback. some have presumed that this must indicate that omi was another lab escape, but i suspect another explanation may better fit: omi was a failed minor sub-mutation that had been around but was going nowhere. then, the vaccines changed the game. the antigens of omi were suddenly highly advantaged and so it spread like wildfire using the fixated immune response of the vaccinated to do so. “would omicron ever have come to prevalence without covid vaccines?” is actually quite an interesting question. (i’m not sure anyone knows for sure)
but it now seems to be evolving rapidly on a pathway that is infecting the most vaxxed most. benefits from boosters are ephemeral at best (and likely mostly derived from bayesian rigging in definitions.) efficacy in case rates rapidly becomes worse than in the twice jabbed or unjabbed.
this issue would be a helluva lot easier to get to the bottom of if we had good data to work with, but country after country is shutting off the series one would need to do accurate work, limiting access, eliminating reporting, and “taking down the data for revision.”
this does not inspire confidence.
“products so effective we cannot allow you to assess their outcomes” is not much of a sales pitch.
simple data like “all cause mortality by vax status, age, and possibly comorbidity” would make straightforward, high confidence analysis easy.
but it seems pretty clear there is little intention of allowing or enabling that.
i fear we’re at the point where such practice must be interpreted with prejudice.
this is too easy a problem to solve to be mishandled so badly by accident at this point, especially as the data that was leading us there all got discontinued and the folks like CDC that are supposed to monitoring VAERS safety signals are refusing to do so.
so we are left triangulating from what we have.
it’s looking more an more to me like the progression of omicron is aggressively becoming highly vaccine enabled. the timing and the outcomes fit on so many separate metrics. this is, unfortunately, precisely the core evolutionary expectation from society scale non-sterilizing immune fixation.
this analysis from the UK is admittedly a little rough and i’d love some input on better ways to clarify the signal/analysis or ways to get at better data, esp ACM by vaxx status rather than using a race proxy.
it feels to me like there is something here but that i have not quite pinned it down to the standard of “high confidence proof.”
let’s get some crowdsourced eyes and minds on this and see if we can figure it out.












Don't forget to factor in Vitamin D levels. They tend to be low in general in populations in more northern countries, but particularly low in those dark skinned who live in northern countries.
To do your study on a population of people that is hardly even affected by the disease and then to vaccinate the controls this was totally designed for us to not have clean data. Then mandating everyone get them so that they don’t have too many unvaxed to send out a crazy signal it all seems so illegal. How are our politicians and lawyers not forcing them to give us this information?